

Impact of human immunodeficiency virus infection on mortality of patients who acquired healthcare associated-infection in critical care unit
- PMID: 31169679
- PMCID: PMC6571254
- DOI: 10.1097/MD.0000000000015801
Impact of human immunodeficiency virus infection on mortality of patients who acquired healthcare associated-infection in critical care unit
Abstract
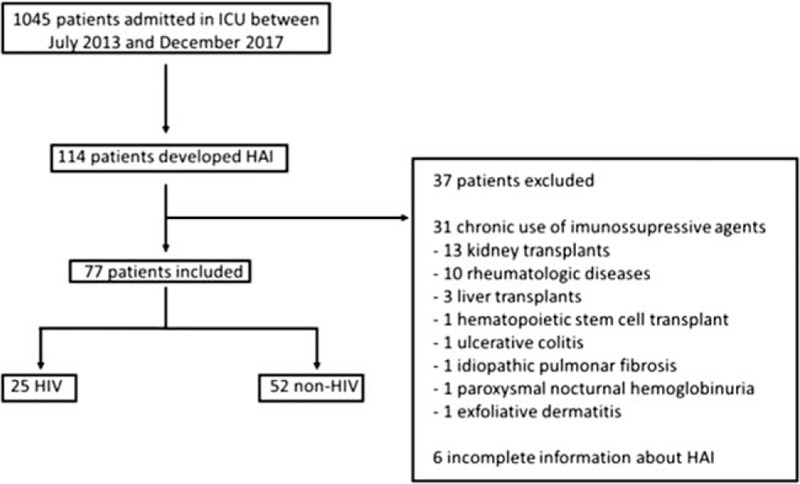
To evaluate 30-day mortality in human immunodeficiency virus (HIV) and non-HIV patients who acquired a healthcare-associated infection (HAI) while in an intensive care unit (ICU), and to describe the epidemiological and microbiological features of HAI in a population with HIV.This was a retrospective cohort study that evaluated patients who acquired HAI during their stay in an Infectious Diseases ICU from July 2013 to December 2017 at a teaching hospital in Brazil.Data were obtained from hospital infection control committee reports and medical records. Statistical analysis was performed using SPSS and a multivariate model was used to evaluate risk factors associated with 30-day mortality. Epidemiological, clinical, and microbiological characteristics of HAI in HIV and non-HIV patients and 30-day mortality were also evaluated.Among 1045 patients, 77 (25 HIV, 52 non-HIV) patients acquired 106 HAI (31 HIV, 75 non-HIV patients). HIV patients were younger (45 vs 58 years, P = .002) and had more respiratory distress than non-HIV patients (60.0% vs 34.6%, P = .035). A high 30-day mortality was observed and there was no difference between groups (HIV, 52.0% vs non-HIV, 54.9%; P = .812). Ventilator-associated pneumonia (VAP) was more frequent in the HIV group compared with the non-HIV group (45.2% vs 26.7%, P = .063), with a predominance of Gram-negative organisms. Gram-positive agents were the most frequent cause of catheter associated-bloodstream infections in HIV patients. Although there was a high frequency of HAI caused by multidrug-resistant organisms (MDRO), no difference was observed between the groups (HIV, 77.8% vs non-HIV, 64.3%; P = .214). Age was the only independent factor associated with 30-day mortality (odds ratio [OR]: 1.05, 95% confidence interval [CI]: 1.01-1.1, P = .017), while diabetes mellitus (OR: 3.64, 95% CI: 0.84-15.8, P = .085) and the Sequential Organ-Failure Assessment (SOFA) score (OR: 1.16, 95% CI: 0.99-1.37, P = .071) had a tendency to be associated with death.HIV infection was not associated with a higher 30-day mortality in critical care patients with a HAI. Age was the only independent risk factor associated with death. VAP was more frequent in HIV patients, probably because of the higher frequency of respiratory conditions at admission, with a predominance of Gram-negative organisms.
Conflict of interest statement
No authors have conflict of interest.
Figures
References
-
- Masur H, Michelis MA, Greene JB, et al. An outbreak of community-acquired Pneumocystis carinii pneumonia: initial manifestation of cellular immune dysfunction. N Engl J Med 1981;305:1431–8. - PubMed
-
- Wachter RM, Luce JM, Turner J, et al. Intensive care of patients with the acquired immunodeficiency syndrome. Outcome and changing patterns of utilization. Am Rev Respir Dis 1986;134:891–6. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998;338:853–60. - PubMed
-
- Maartens G, Celum C, Lewin SR. HIV infection: epidemiology, pathogenesis, treatment, and prevention. Lancet 2014;384:258–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
