

One-way SMS and healthcare outcomes in Africa: Systematic review of randomised trials with meta-analysis
- PMID: 31170176
- PMCID: PMC6553734
- DOI: 10.1371/journal.pone.0217485
One-way SMS and healthcare outcomes in Africa: Systematic review of randomised trials with meta-analysis
Abstract
Background: The impact of one-way SMS on health outcomes in Africa is unclear. We aimed to conduct a systematic review of one-way SMS randomised trials in Africa and a meta-analysis of their effect on healthcare appointments attendance and medicine adherence.
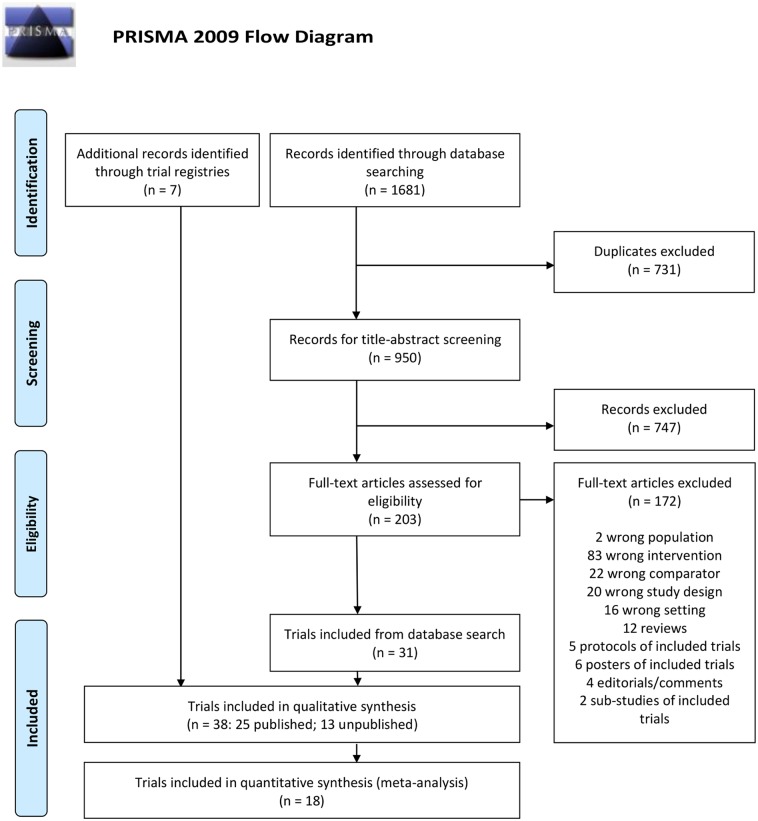
Methods: PubMed, Embase, CENTRAL, The Global Health Library, ClinicalTrials.gov, ICTRP, and PACTR were searched for published and unpublished trials in Africa without language restriction (up to April 2018). Trials reporting effect estimates on healthcare appointment attendance and medicine adherence were assessed for risk of bias and included in meta-analyses using random-effects models. Other outcomes were reported descriptively. The protocol is registered in PROSPERO, ID:CRD42018081062.
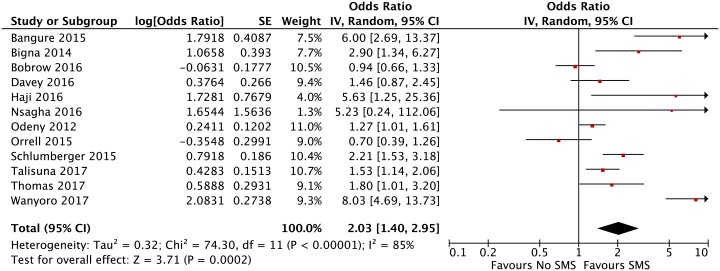
Results: We included 38 one-way SMS trials conducted in Africa within a broad range of clinical conditions. Eighteen trials were included in the meta-analyses, and four were assessed as overall low risk of bias. One-way SMS improved appointment attendance, OR:2·03; 95% CI:1·40-2·95 (12 trials, 6448 participants), but not medicine adherence, RR:1·10; 95% CI:0·98-1·23 (nine trials, 4213 participants). Subgroup analyses showed that one-way SMS had the highest impact on childhood immunization attendance, OR:3·69; 95% CI:1·67-8·13 (three trials, 1943 participants). There was no clear evidence of one-way SMS improving facility delivery, knowledge level (reproductive/antenatal health, hypertension), diabetes- and hypertension management.
Conclusion: In an African setting, the clinical effect of one-way SMS is uncertain except for appointment attendance where the effect seems to vary depending on which clinical condition it is used in.
Conflict of interest statement
DSL, VR, MSA are currently conducting a trial in Tanzania assessing the effect of one-way SMS on attendance to cervical cancer screening follow-up appointment attendance. This does not alter our adherence to PLOS ONE policies on data sharing and materials. AL, MK and JK have no conflicts of interest.
Figures



References
-
- World Bank. World Development Report 2016: Digital Dividends. Washington DC: World Bank, 2016.
-
- World Health Organization. Global diffusion of eHealth: Making universal health coverage achievable Report of the third global survey on eHealth. Geneva: World Health Organization, 2016.
-
- Qiang C, Yamamichi M, Hausman V, Miller R, Altman D. Mobile Applications for the Health Sector. Washington DC: World Bank, 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
