

Differential Poststroke Motor Recovery in an Arm Versus Hand Muscle in the Absence of Motor Evoked Potentials
- PMID: 31170880
- PMCID: PMC6631316
- DOI: 10.1177/1545968319850138
Differential Poststroke Motor Recovery in an Arm Versus Hand Muscle in the Absence of Motor Evoked Potentials
Abstract
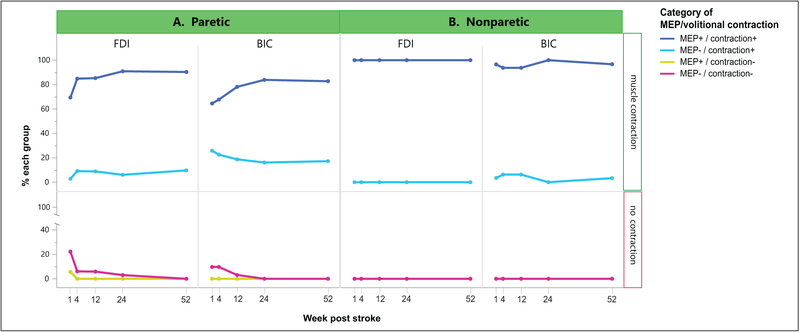
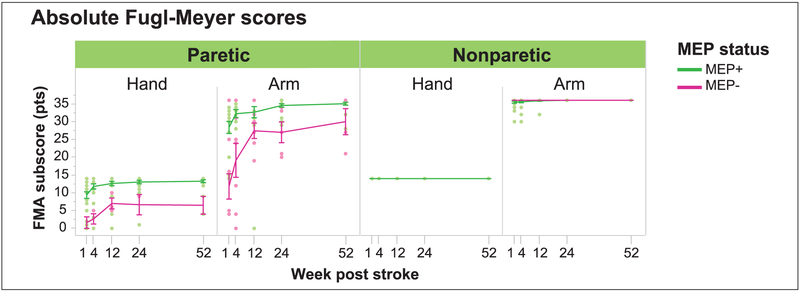
Background. After stroke, recovery of movement in proximal and distal upper extremity (UE) muscles appears to follow different time courses, suggesting differences in their neural substrates. Objective. We sought to determine if presence or absence of motor evoked potentials (MEPs) differentially influences recovery of volitional contraction and strength in an arm muscle versus an intrinsic hand muscle. We also related MEP status to recovery of proximal and distal interjoint coordination and movement fractionation, as measured by the Fugl-Meyer Assessment (FMA). Methods. In 45 subjects in the year following ischemic stroke, we tracked the relationship between corticospinal tract (CST) integrity and behavioral recovery in the biceps (BIC) and first dorsal interosseous (FDI) muscle. We used transcranial magnetic stimulation to probe CST integrity, indicated by MEPs, in BIC and FDI. We used electromyography, dynamometry, and UE FMA subscores to assess muscle-specific contraction, strength, and inter-joint coordination, respectively. Results. Presence of MEPs resulted in higher likelihood of muscle contraction, greater strength, and higher FMA scores. Without MEPs, BICs could more often volitionally contract, were less weak, and had steeper strength recovery curves than FDIs; in contrast, FMA recovery curves plateaued below normal levels for both the arm and hand. Conclusions. There are shared and separate substrates for paretic UE recovery. CST integrity is necessary for interjoint coordination in both segments and for overall recovery. In its absence, alternative pathways may assist recovery of volitional contraction and strength, particularly in BIC. These findings suggest that more targeted approaches might be needed to optimize UE recovery.
Keywords: motor cortex; motor evoked potential; neurorehabilitation; stroke recovery; transcranial magnetic stimulation.
Conflict of interest statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


Similar articles
-
Predicting hand motor recovery in severe stroke: the role of motor evoked potentials in relation to early clinical assessment.Neurorehabil Neural Repair. 2009 Jan;23(1):45-51. doi: 10.1177/1545968308317578. Epub 2008 Sep 15. Neurorehabil Neural Repair. 2009. PMID: 18794218
-
Neural Substrates of Motor Recovery in Severely Impaired Stroke Patients With Hand Paralysis.Neurorehabil Neural Repair. 2016 May;30(4):328-38. doi: 10.1177/1545968315594886. Epub 2015 Jul 10. Neurorehabil Neural Repair. 2016. PMID: 26163204 Free PMC article.
-
Corticoreticulospinal tract neurophysiology in an arm and hand muscle in healthy and stroke subjects.J Physiol. 2021 Aug;599(16):3955-3971. doi: 10.1113/JP281681. J Physiol. 2021. PMID: 34229359 Free PMC article.
-
Prediction of motor recovery after stroke: being pragmatic or innovative?Curr Opin Neurol. 2020 Aug;33(4):482-487. doi: 10.1097/WCO.0000000000000843. Curr Opin Neurol. 2020. PMID: 32657889 Review.
-
Corticomotor pathway function and recovery after stroke: a look back and a way forward.J Physiol. 2025 Feb;603(3):651-662. doi: 10.1113/JP285562. Epub 2024 May 30. J Physiol. 2025. PMID: 38814805 Free PMC article. Review.
Cited by
-
Data-Driven Quantitation of Movement Abnormality after Stroke.Bioengineering (Basel). 2023 May 26;10(6):648. doi: 10.3390/bioengineering10060648. Bioengineering (Basel). 2023. PMID: 37370579 Free PMC article.
-
Clinical diagnostic utility of transcranial magnetic stimulation in neurological disorders. Updated report of an IFCN committee.Clin Neurophysiol. 2023 Jun;150:131-175. doi: 10.1016/j.clinph.2023.03.010. Epub 2023 Mar 29. Clin Neurophysiol. 2023. PMID: 37068329 Free PMC article. Review.
-
The Strength of the Corticospinal Tract Not the Reticulospinal Tract Determines Upper-Limb Impairment Level and Capacity for Skill-Acquisition in the Sub-Acute Post-Stroke Period.Neurorehabil Neural Repair. 2021 Sep;35(9):812-822. doi: 10.1177/15459683211028243. Epub 2021 Jul 4. Neurorehabil Neural Repair. 2021. PMID: 34219510 Free PMC article.
-
Corticospinal and corticoreticulospinal projections have discrete but complementary roles in chronic motor behaviors after stroke.J Neurophysiol. 2024 Dec 1;132(6):1917-1936. doi: 10.1152/jn.00301.2024. Epub 2024 Nov 6. J Neurophysiol. 2024. PMID: 39503588
-
Stroke Lesion Volume and Injury to Motor Cortex Output Determines Extent of Contralesional Motor Cortex Reorganization.Neurorehabil Neural Repair. 2023 Feb-Mar;37(2-3):119-130. doi: 10.1177/15459683231152816. Epub 2023 Feb 14. Neurorehabil Neural Repair. 2023. PMID: 36786394 Free PMC article.
References
-
- Twitchell TE. The restoration of motor function following hemiplegia in man. Brain. 1951;74:443–480. - PubMed
-
- Colebatch JG, Gandevia SC. The distribution of muscular weakness in upper motor neuron lesions affecting the arm. Brain. 1989;112(pt 3):749–763. - PubMed
-
- Lawrence DG, Kuypers HG. The functional organization of the motor system in the monkey. II. The effects of lesions of the descending brain-stem pathways. Brain. 1968;91:15–36. - PubMed
-
- Lawrence DG, Kuypers HG. The functional organization of the motor system in the monkey. I. The effects of bilateral pyramidal lesions. Brain. 1968;91:1–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
