

Final analyses of OPTiM: a randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III-IV melanoma
- PMID: 31171039
- PMCID: PMC6554874
- DOI: 10.1186/s40425-019-0623-z
Final analyses of OPTiM: a randomized phase III trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in unresectable stage III-IV melanoma
Abstract
Background: Talimogene laherparepvec is an oncolytic immunotherapy approved in the US, Europe, Australia and Switzerland. We report the final planned analysis of OPTiM, a randomized open-label phase III trial in patients with unresectable stage IIIB-IVM1c melanoma.
Methods: Patients were randomized 2:1 to receive intratumoral talimogene laherparepvec or subcutaneous recombinant GM-CSF. In addition to overall survival (OS), durable response rate (DRR), objective response rate (ORR), complete responses (CR), and safety are also reported. All final analyses are considered to be descriptive and treatment responses were assessed by the investigators.
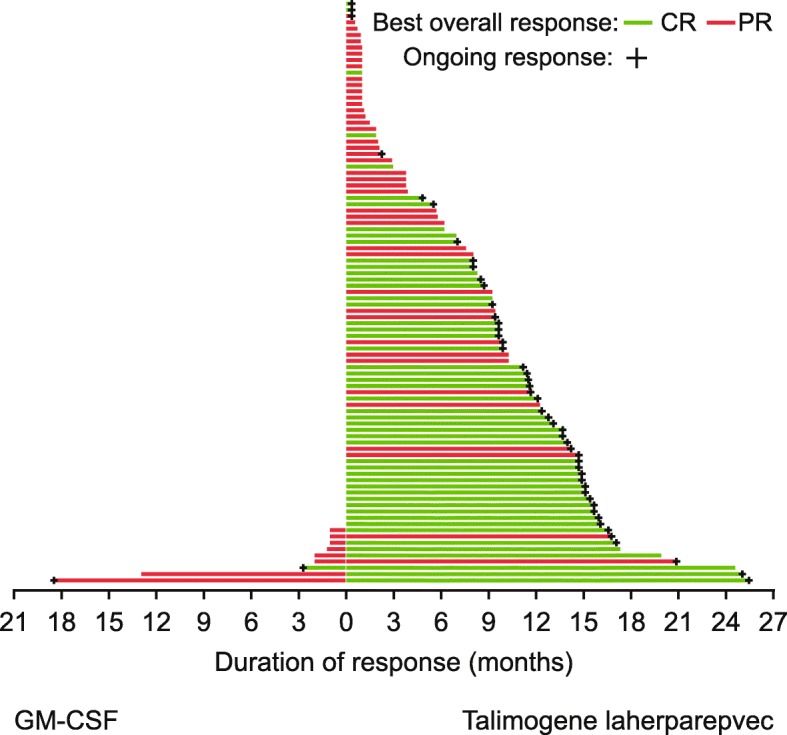
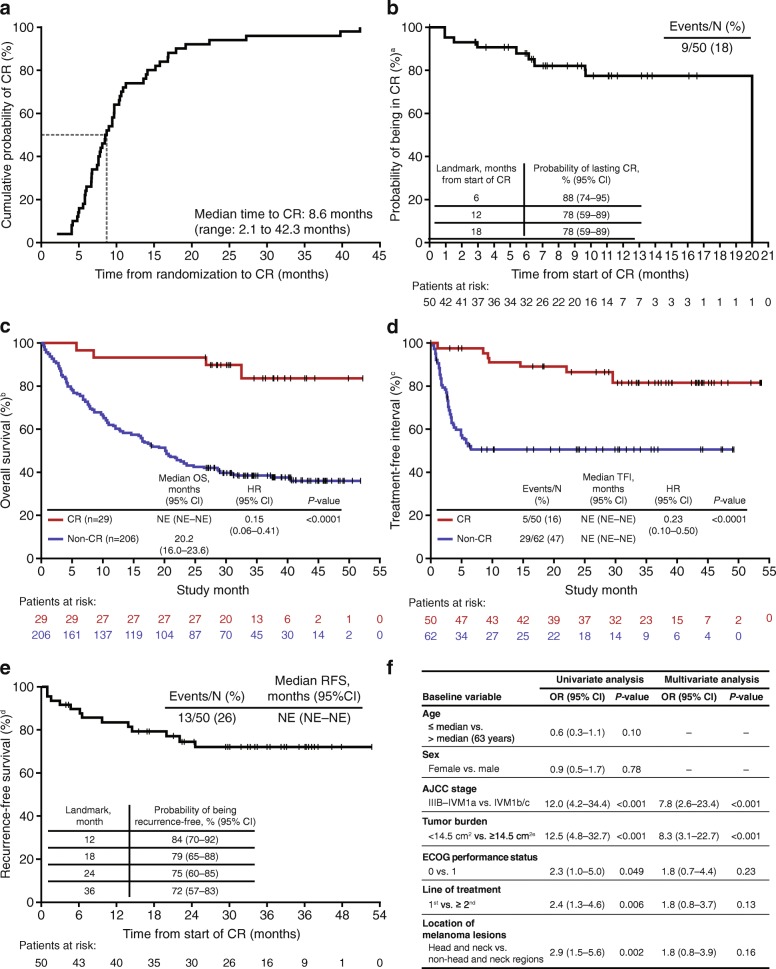
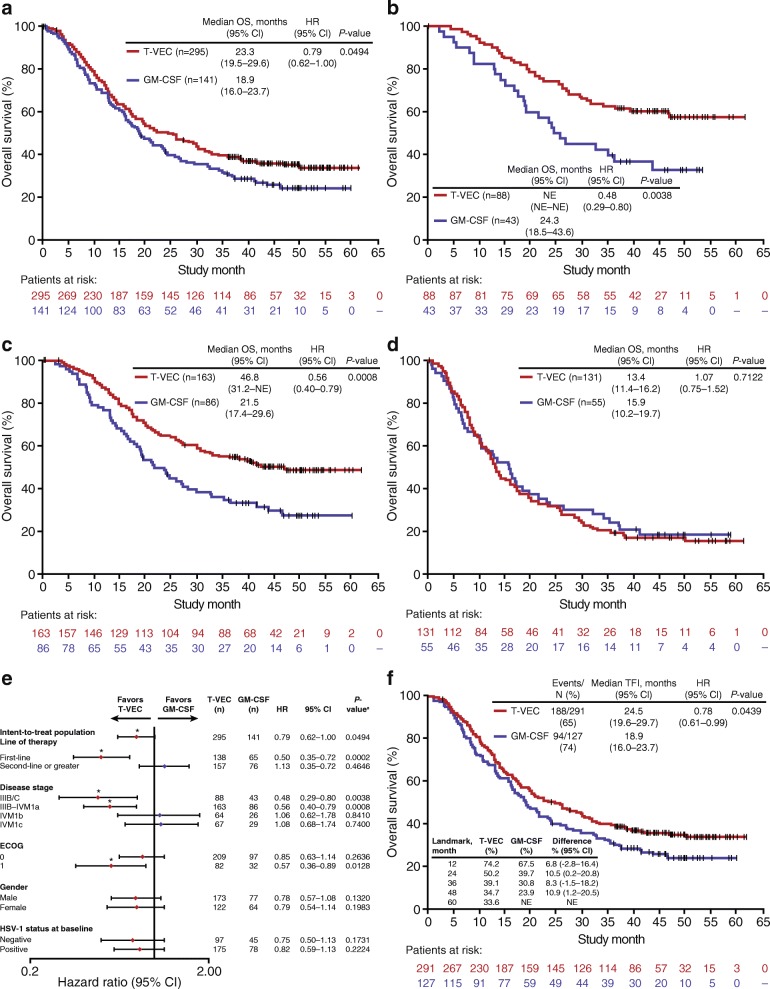
Results: Of 436 patients in the intent-to-treat population, 295 were allocated to talimogene laherparepvec and 141 to GM-CSF. Median follow-up in the final OS analysis was 49 months. Median OS was 23.3 months (95% confidence interval [CI], 19.5-29.6) and 18.9 months (95% CI, 16.0-23.7) in the talimogene laherparepvec and GM-CSF arms, respectively (unstratified hazard ratio, 0.79; 95% CI, 0.62-1.00; p = 0.0494 [descriptive]). DRR was 19.0 and 1.4% (unadjusted odds ratio, 16.6; 95% CI, 4.0-69.2; p < 0.0001); ORR was 31.5 and 6.4%. Fifty (16.9%) and 1 (0.7%) patient in the talimogene laherparepvec and GM-CSF arms, respectively, achieved CR. In talimogene laherparepvec-treated patients, median time to CR was 8.6 months; median CR duration was not reached. Among patients with a CR, 88.5% were estimated to survive at a 5-year landmark analysis. Talimogene laherparepvec efficacy was more pronounced in stage IIIB-IVM1a melanoma as already described in the primary analysis. The safety reporting was consistent with the primary OPTiM analysis.
Conclusions: In this final planned OPTiM analysis, talimogene laherparepvec continued to result in improved longer-term efficacy versus GM-CSF and remained well tolerated. The final analysis also confirms that talimogene laherparepvec was associated with durable CRs that were associated with prolonged survival.
Trial registration: ClinicalTrials.gov identifier: NCT00769704 .
Keywords: Efficacy; Final analysis; Melanoma; Overall survival; Talimogene laherparepvec.
Conflict of interest statement
Figures
References
-
- U. S. Food and Drug Administration . Imlygic (talimogene laherparepvec) prescribing information. 2015.
-
- Harrington KJ, Andtbacka RH, Collichio F, Downey G, Chen L, Szabo Z, et al. Efficacy and safety of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor in patients with stage IIIB/C and IVM1a melanoma: subanalysis of the phase III OPTiM trial. Onco Targets Ther. 2016;9:7081–7093. doi: 10.2147/OTT.S115245. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical