

Combined BRAF and MEK inhibition with PD-1 blockade immunotherapy in BRAF-mutant melanoma
- PMID: 31171879
- PMCID: PMC8562134
- DOI: 10.1038/s41591-019-0476-5
Combined BRAF and MEK inhibition with PD-1 blockade immunotherapy in BRAF-mutant melanoma
Erratum in
-
Publisher Correction: Combined BRAF and MEK inhibition with PD-1 blockade immunotherapy in BRAF-mutant melanoma.Nat Med. 2019 Aug;25(8):1319. doi: 10.1038/s41591-019-0535-y. Nat Med. 2019. PMID: 31267021
Abstract
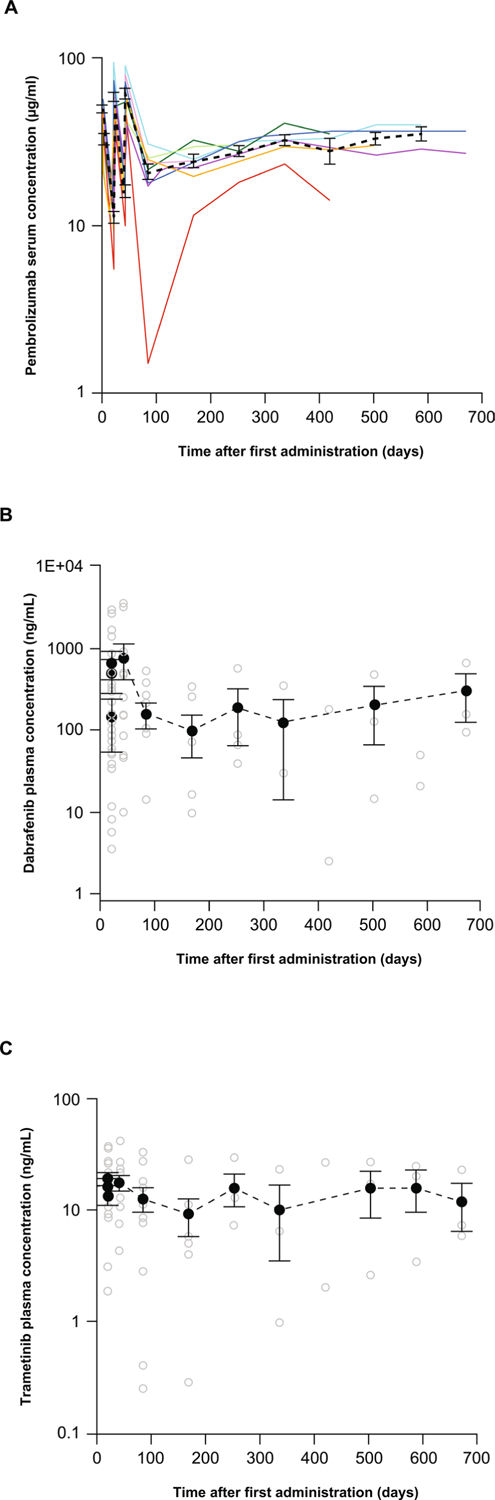
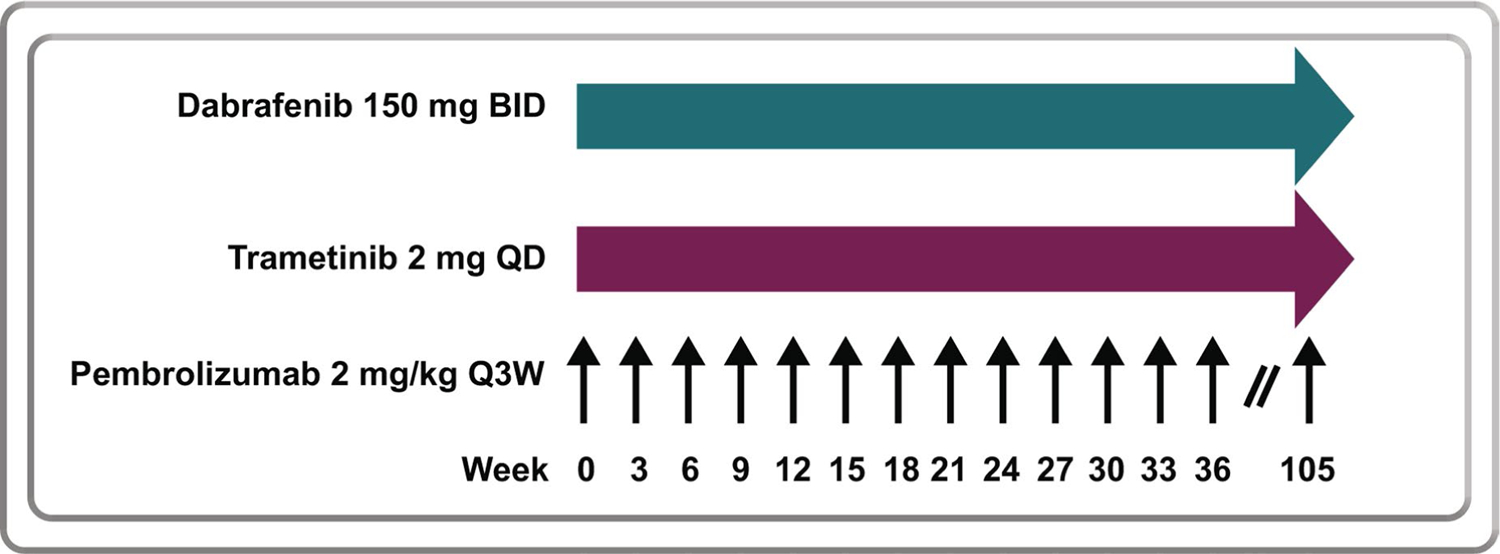
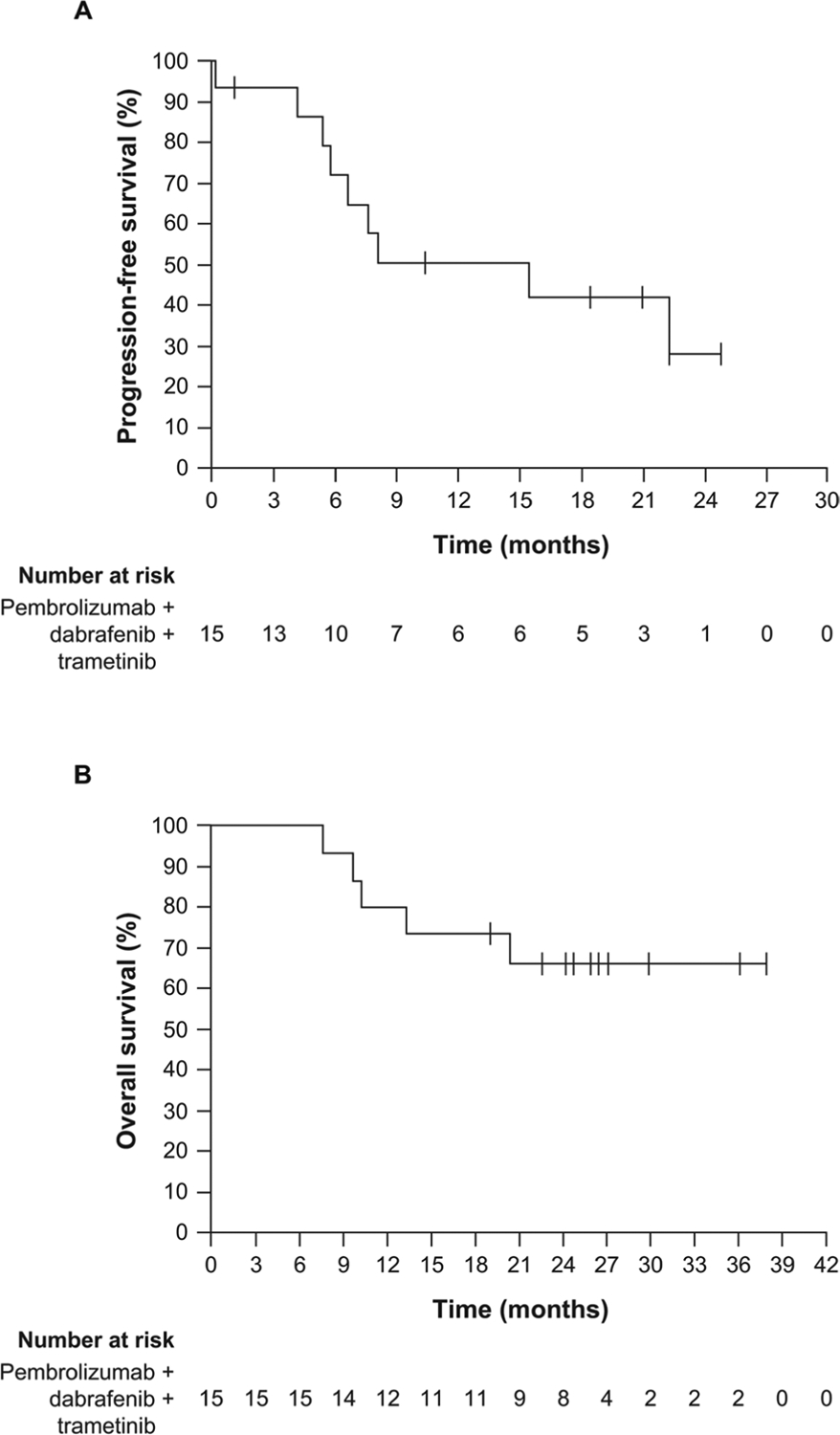
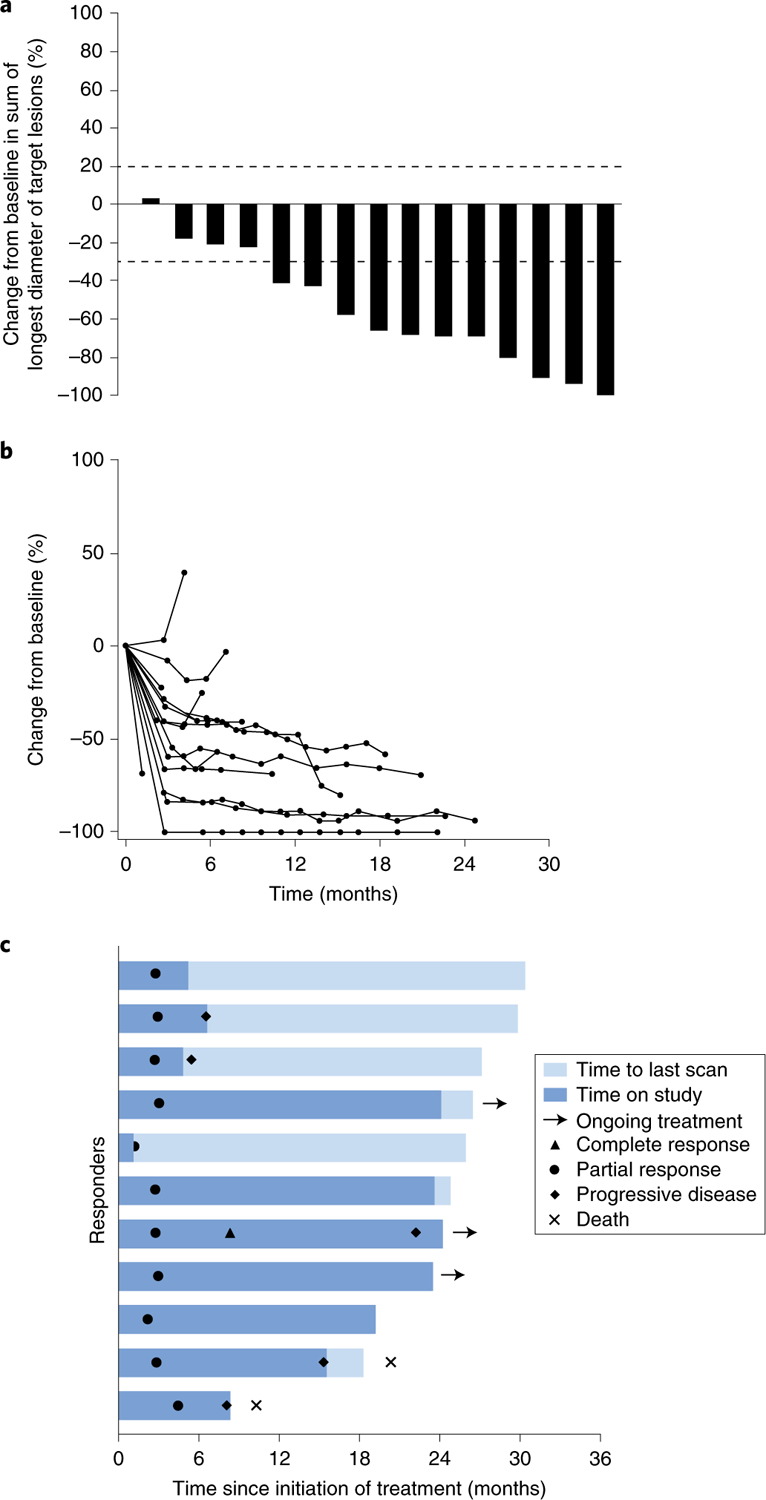
Oncogene-targeted therapy with B-Raf proto-oncogene (BRAF) and mitogen-activated protein kinase kinase (MEK) inhibitors induces a high initial response rate in patients with BRAFV600-mutated melanoma, with a median duration of response of approximately 1 year1-3. Immunotherapy with antibodies to programmed death 1 (PD-1) produces lower response rates but with long response duration. Preclinical models suggest that combining BRAF and MEK inhibitors with PD-1 blockade therapy improves antitumor activity4-6, which may provide additional treatment options for patients unlikely to have long-lasting responses to either mode of therapy alone. We enrolled 15 patients with BRAFV600-mutated metastatic melanoma in a first-in-human clinical trial of dabrafenib, trametinib and pembrolizumab ( NCT02130466 ). Eleven patients (73%) experienced grade 3/4 treatment-related adverse events, the most common being elevation of liver function tests and pyrexia, most of which resolved with drug interruption or discontinuation of either the anti-PD-1 antibody or the targeted therapy combination. Eleven patients (73%; 95% confidence interval = 45-92%) had an objective response, and six (40%; 95% confidence interval = 16-68%) continued with a response at a median follow-up of 27 months (range = 10.3-38.4+ months) for all patients. This study suggests that this triple-combined therapy may benefit a subset of patients with BRAFV600-mutated metastatic melanoma by increasing the frequency of long-lasting antitumor responses.
Figures
Comment in
-
Combining checkpoint inhibition and targeted therapy in melanoma.Nat Med. 2019 Jun;25(6):879-882. doi: 10.1038/s41591-019-0482-7. Nat Med. 2019. PMID: 31171877 No abstract available.
-
BRAF+MEKi and ICI triplets show promise in melanoma.Nat Rev Clin Oncol. 2019 Sep;16(9):525. doi: 10.1038/s41571-019-0247-8. Nat Rev Clin Oncol. 2019. PMID: 31239555 No abstract available.
References
-
- Larkin J et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N. Engl. J. Med 371, 1867–1876 (2014). - PubMed
-
- Long GV et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N. Engl. J. Med 371, 1877–1888 (2014). - PubMed
-
- Robert C et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med 372, 30–39 (2015). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
