

Systematically profiling the expression of eIF3 subunits in glioma reveals the expression of eIF3i has prognostic value in IDH-mutant lower grade glioma
- PMID: 31171919
- PMCID: PMC6549376
- DOI: 10.1186/s12935-019-0867-1
Systematically profiling the expression of eIF3 subunits in glioma reveals the expression of eIF3i has prognostic value in IDH-mutant lower grade glioma
Abstract
Background: Abnormal expression of the eukaryotic initiation factor 3 (eIF3) subunits plays critical roles in tumorigenesis and progression, and also has potential prognostic value in cancers. However, the expression and clinical implications of eIF3 subunits in glioma remain unknown.
Methods: Expression data of eIF3 for patients with gliomas were obtained from the Chinese Glioma Genome Atlas (CGGA) (n = 272) and The Cancer Genome Atlas (TCGA) (n = 595). Cox regression, the receiver operating characteristic (ROC) curves and Kaplan-Meier analysis were used to study the prognostic value. Gene oncology (GO) and gene set enrichment analysis (GSEA) were utilized for functional prediction.
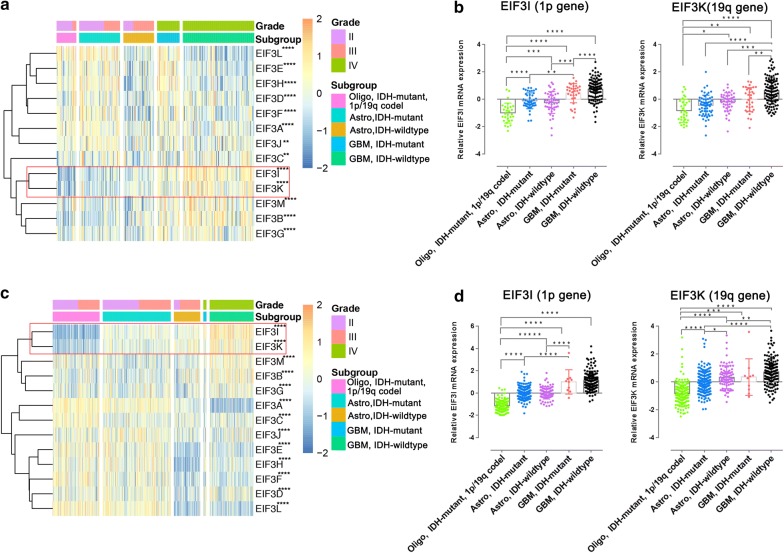
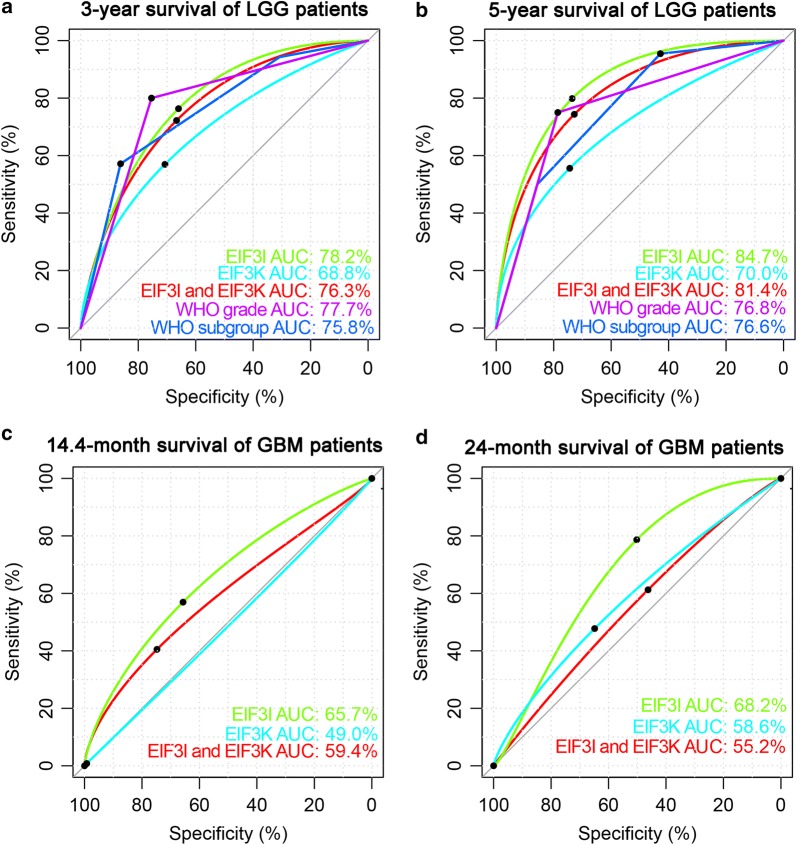
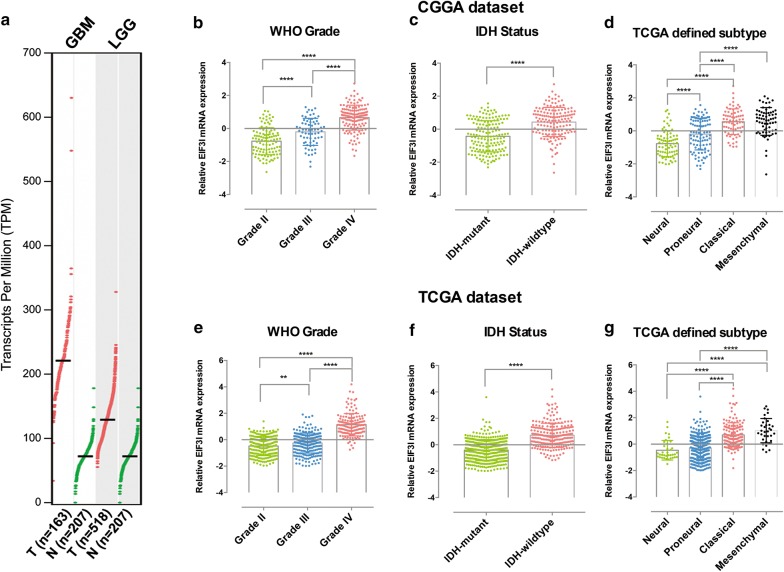
Results: In both the CGGA and TCGA datasets, the expression levels of eIF3d, eIF3e, eIF3f, eIF3h and eIF3l highly were associated with the IDH mutant status of gliomas. The expression of eIF3b, eIF3i, eIF3k and eIF3m was increased with the tumor grade, and was associated with poorer overall survival [All Hazard ratio (HR) > 1 and P < 0.05]. By contrast, the expression of eIF3a and eIF3l was decreased in higher grade gliomas and was associated with better overall survival (Both HR < 1 and P < 0.05). Importantly, the expression of eIF3i (located on chromosome 1p) and eIF3k (Located on chromosome 19q) were the two highest risk factors in both the CGGA [eIF3i HR = 2.068 (1.425-3.000); eIF3k HR = 1.737 (1.166-2.588)] and TCGA [eIF3i HR = 1.841 (1.642-2.064); eIF3k HR = 1.521 (1.340-1.726)] databases. Among eIF3i, eIF3k alone or in combination, the expression of eIF3i was the more robust in stratifying the survival of glioma in various pathological subgroups. The expression of eIF3i was an independent prognostic factor in IDH-mutant lower grade glioma (LGG) and could also predict the 1p/19q codeletion status of IDH-mutant LGG. Finally, GO and GSEA analysis showed that the elevated expression of eIF3i was significantly correlated with the biological processes of cell proliferation, mRNA processing, translation, T cell receptor signaling, NF-κB signaling and others.
Conclusions: Our study reveals the expression alterations during glioma progression, and highlights the prognostic value of eIF3i in IDH-mutant LGG.
Keywords: 1p/19q codeletion; Biomarker; Glioma; Prognosis; eIF3.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures


References
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
