

The primacy of multiparametric MRI in men with suspected prostate cancer
- PMID: 31172275
- PMCID: PMC6828624
- DOI: 10.1007/s00330-019-06166-z
The primacy of multiparametric MRI in men with suspected prostate cancer
Abstract
Background: Multiparametric MRI (mpMRI) became recognised in investigating those with suspected prostate cancer between 2010 and 2012; in the USA, the preventative task force moratorium on PSA screening was a strong catalyst. In a few short years, it has been adopted into daily urological and oncological practice. The pace of clinical uptake, born along by countless papers proclaiming high accuracy in detecting clinically significant prostate cancer, has sparked much debate about the timing of mpMRI within the traditional biopsy-driven clinical pathways. There are strongly held opposing views on using mpMRI as a triage test regarding the need for biopsy and/or guiding the biopsy pattern.
Objective: To review the evidence base and present a position paper on the role of mpMRI in the diagnosis and management of prostate cancer.
Methods: A subgroup of experts from the ESUR Prostate MRI Working Group conducted literature review and face to face and electronic exchanges to draw up a position statement.
Results: This paper considers diagnostic strategies for clinically significant prostate cancer; current national and international guidance; the impact of pre-biopsy mpMRI in detection of clinically significant and clinically insignificant neoplasms; the impact of pre-biopsy mpMRI on biopsy strategies and targeting; the notion of mpMRI within a wider risk evaluation on a patient by patient basis; the problems that beset mpMRI including inter-observer variability.
Conclusions: The paper concludes with a set of suggestions for using mpMRI to influence who to biopsy and who not to biopsy at diagnosis.
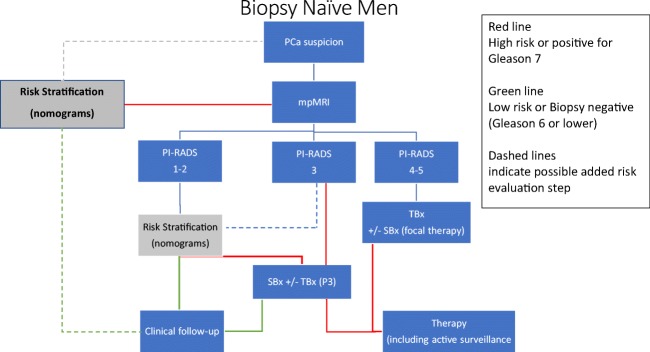
Key points: • Adopt mpMRI as the first, and primary, investigation in the workup of men with suspected prostate cancer. • PI-RADS assessment categories 1 and 2 have a high negative predictive value in excluding significant disease, and systematic biopsy may be postponed, especially in men with low-risk of disease following additional risk stratification. • PI-RADS assessment category lesions 4 and 5 should be targeted; PI-RADS assessment category lesion 3 may be biopsied as a target, as part of systematic biopsies or may be observed depending on risk stratification.
Keywords: Biopsy; Magnetic resonance imaging; Observer variation; Prostate cancer; Risk assessment.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
-
- Mottet N, van den Bergh RCN, Briers E et al (2018) Guidelines on prostate cancer. https://uroweb.org/guideline/prostate-cancer/?type=archive
-
- Linson PW, Lee AK, Doytchinova T, et al. Percentage of core lengths involved with prostate cancer: does it add to the percentage of positive prostate biopsies in predicting postoperative prostate-specific antigen outcome for men with intermediate-risk prostate cancer. Urology. 2002;59:704–708. doi: 10.1016/S0090-4295(01)01665-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
