

Efficacy and Prognosis of 3D Printing Technology in Treatment of High-Energy Trans-Syndesmotic Ankle Fracture Dislocation - "Log-Splitter" Injury
- PMID: 31172985
- PMCID: PMC6572869
- DOI: 10.12659/MSM.916884
Efficacy and Prognosis of 3D Printing Technology in Treatment of High-Energy Trans-Syndesmotic Ankle Fracture Dislocation - "Log-Splitter" Injury
Abstract
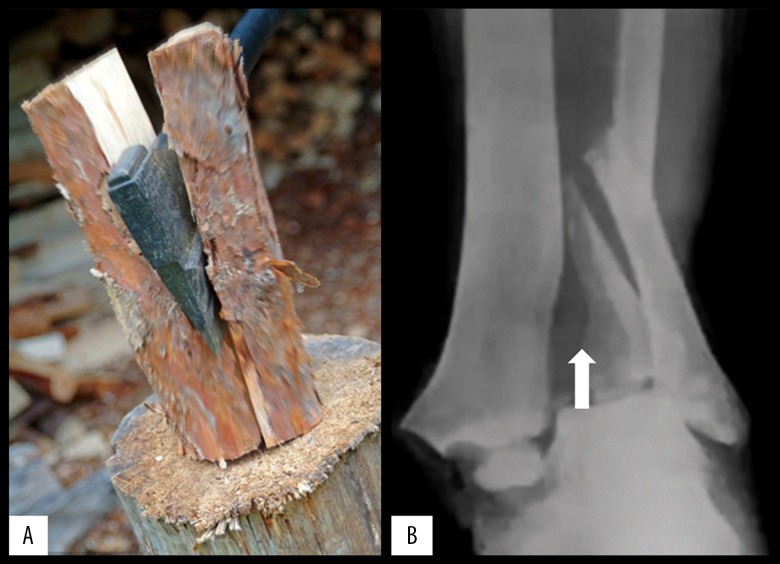
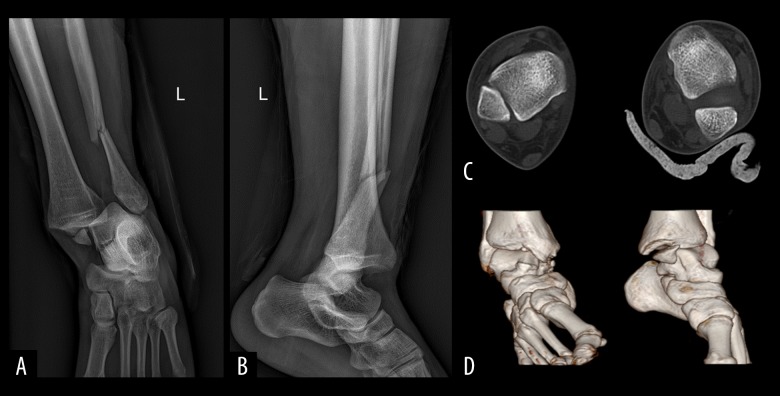
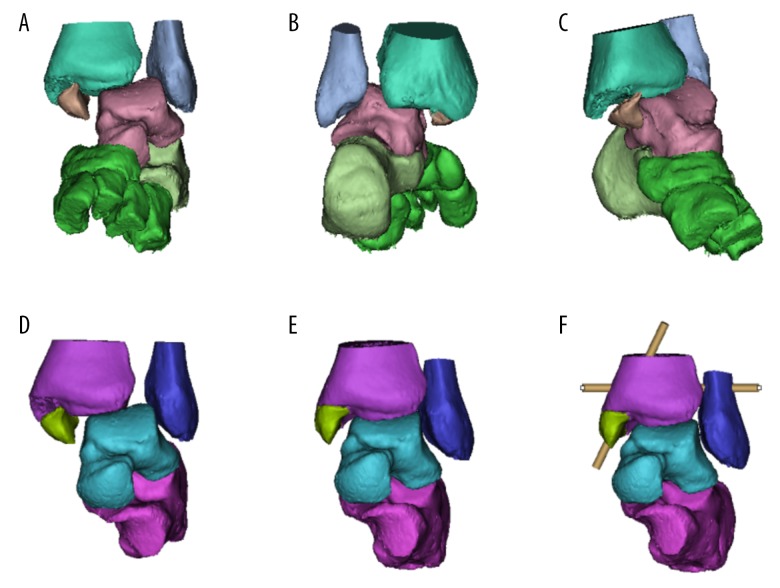
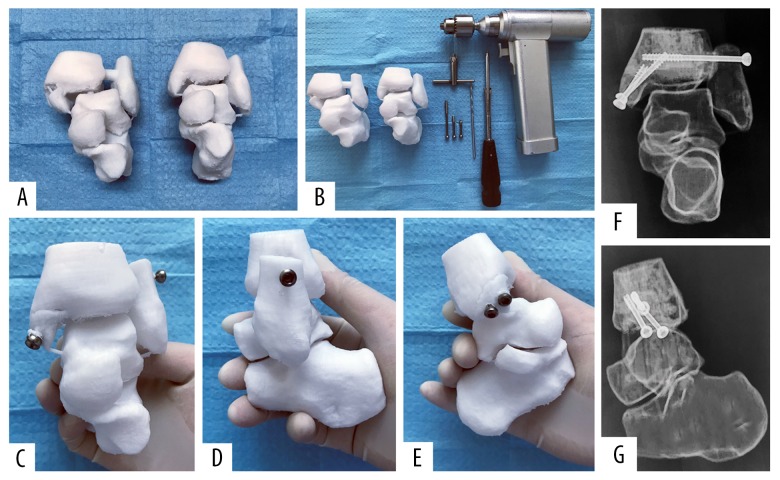
BACKGROUND This study aimed to retrospectively assess the feasibility and efficacy of three-dimensional (3D) printing technology in the treatment of high-energy trans-syndesmotic ankle fracture dislocation - "log-splitter" injury - and to evaluate the efficacy and prognosis. MATERIAL AND METHODS We included 29 patients (17 males and 12 females; mean age, 44.0±13.2 years) with log-splitter injury from June 2011 to December 2016, divided into a routine group (n=13) and a 3D printing group (n=16) according to the surgical method used. Operation time, intraoperative blood loss, fluoroscopy times, fracture union time, functional outcomes based on AOFAS (American Orthopedic Foot and Ankle Society) score, and postoperative complications were observed and recorded. RESULTS Compared with the routine treatment group, 3D printing technology had better safety and efficacy for the treatment of log-splitter injury and the advantages of shorter operation time, less intraoperative blood loss, fewer fluoroscopies needed, and higher rate of good functional outcome (P<0.001, P<0.001, P<0.001, and P=0.017, respectively). However, no significant difference was noted in the rate of anatomical reduction, mean AOFAS score at the last follow-up (mean time, 19.9±2.8 months), or postoperative complications between the 2 groups (P=0.370, P=0.156, and P=0.485, respectively). CONCLUSIONS Surgery assisted by 3D printing technology to treat log-splitter injury is feasible and effective, and may be a good optional approach to formulate a reasonable personalized surgical plan and to optimize the outcomes.
Conflict of interest statement
None.
Figures
References
-
- Salai M, Dudkiewicz I, Novikov I, et al. The epidemic of ankle fractures in the elderly – is surgical treatment warranted? Arch Orthop Trauma Surg. 2000;120(9):511–13. - PubMed
-
- McCollum GA, van den Bekerom MP, Kerkhoffs GM, et al. Syndesmosis and deltoid ligament injuries in the athlete. Knee Surg Sports Traumatol Arthrosc. 2013;21(6):1328–37. - PubMed
-
- Weening B, Bhandari M. Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma. 2005;19(2):102–8. - PubMed
-
- Fallat L, Grimm DJ, Saracco JA. Sprained ankle syndrome: Prevalence and analysis of 639 acute injuries. J Foot Ankle Surg. 1998;37(4):280–85. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
