

Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults
- PMID: 31173647
- PMCID: PMC6555588
- DOI: 10.1002/14651858.CD009593.pub4
Xpert MTB/RIF and Xpert MTB/RIF Ultra for pulmonary tuberculosis and rifampicin resistance in adults
Update in
-
Xpert Ultra versus Xpert MTB/RIF for pulmonary tuberculosis and rifampicin resistance in adults with presumptive pulmonary tuberculosis.Cochrane Database Syst Rev. 2021 Feb 22;2(2):CD009593. doi: 10.1002/14651858.CD009593.pub5. Cochrane Database Syst Rev. 2021. PMID: 33616229 Free PMC article.
Abstract
Background: Xpert MTB/RIF (Xpert MTB/RIF) and Xpert MTB/RIF Ultra (Xpert Ultra), the newest version, are the only World Health Organization (WHO)-recommended rapid tests that simultaneously detect tuberculosis and rifampicin resistance in persons with signs and symptoms of tuberculosis, at lower health system levels. A previous Cochrane Review found Xpert MTB/RIF sensitive and specific for tuberculosis (Steingart 2014). Since the previous review, new studies have been published. We performed a review update for an upcoming WHO policy review.
Objectives: To determine diagnostic accuracy of Xpert MTB/RIF and Xpert Ultra for tuberculosis in adults with presumptive pulmonary tuberculosis (PTB) and for rifampicin resistance in adults with presumptive rifampicin-resistant tuberculosis.
Search methods: We searched the Cochrane Infectious Diseases Group Specialized Register, MEDLINE, Embase, Science Citation Index, Web of Science, Latin American Caribbean Health Sciences Literature, Scopus, the WHO International Clinical Trials Registry Platform, the International Standard Randomized Controlled Trial Number Registry, and ProQuest, to 11 October 2018, without language restriction.
Selection criteria: Randomized trials, cross-sectional, and cohort studies using respiratory specimens that evaluated Xpert MTB/RIF, Xpert Ultra, or both against the reference standard, culture for tuberculosis and culture-based drug susceptibility testing or MTBDRplus for rifampicin resistance.
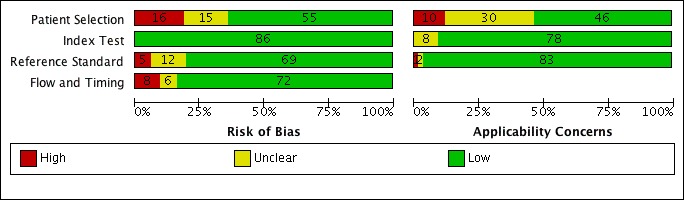
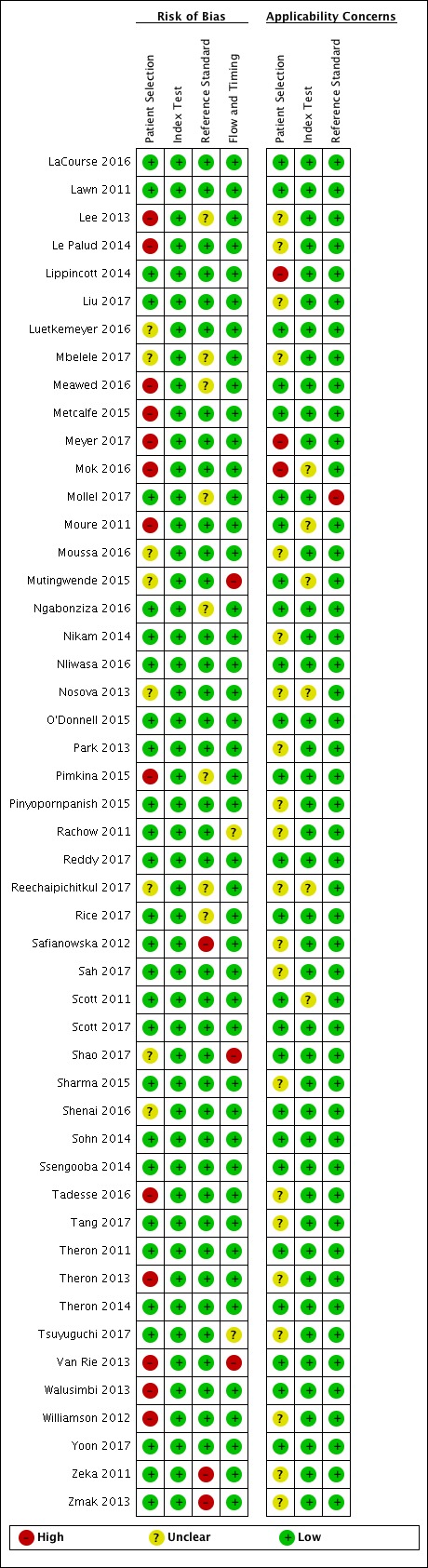
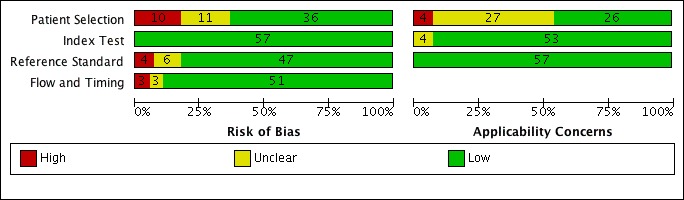
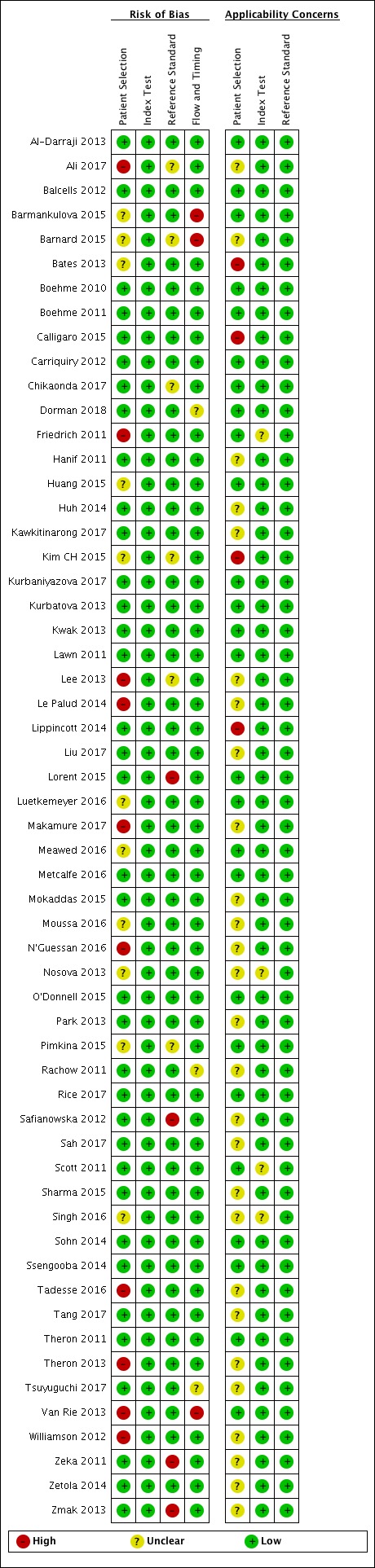
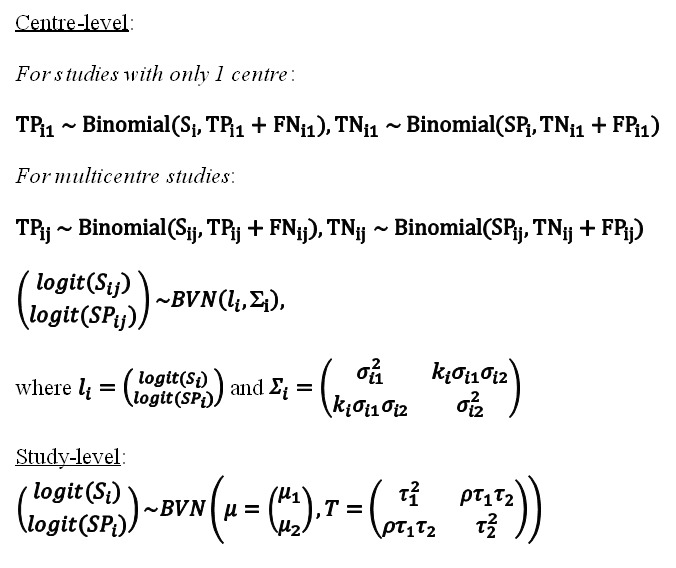
Data collection and analysis: Four review authors independently extracted data using a standardized form. When possible, we also extracted data by smear and HIV status. We assessed study quality using QUADAS-2 and performed meta-analyses to estimate pooled sensitivity and specificity separately for tuberculosis and rifampicin resistance. We investigated potential sources of heterogeneity. Most analyses used a bivariate random-effects model. For tuberculosis detection, we first estimated accuracy using all included studies and then only the subset of studies where participants were unselected, i.e. not selected based on prior microscopy testing.
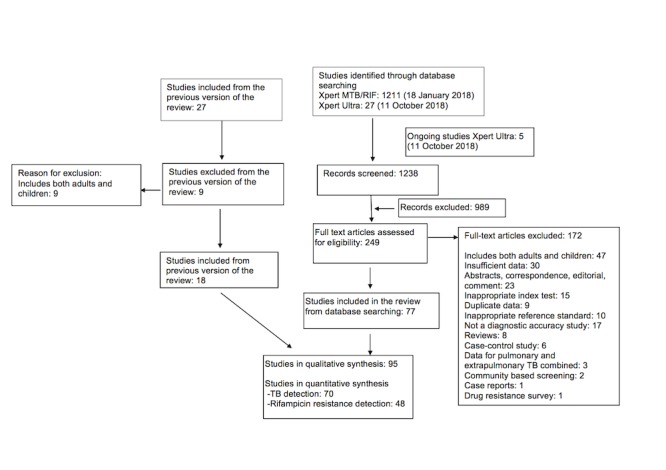
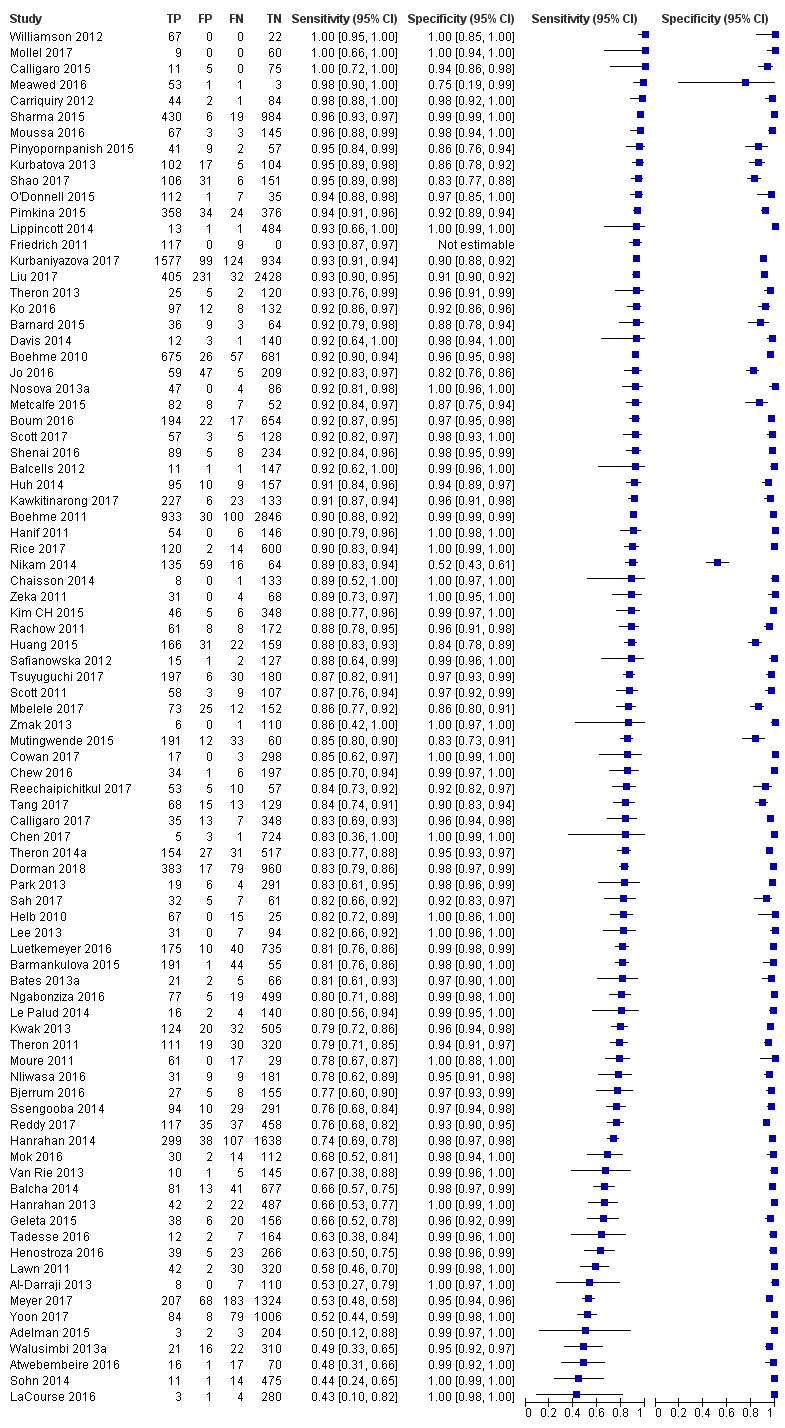
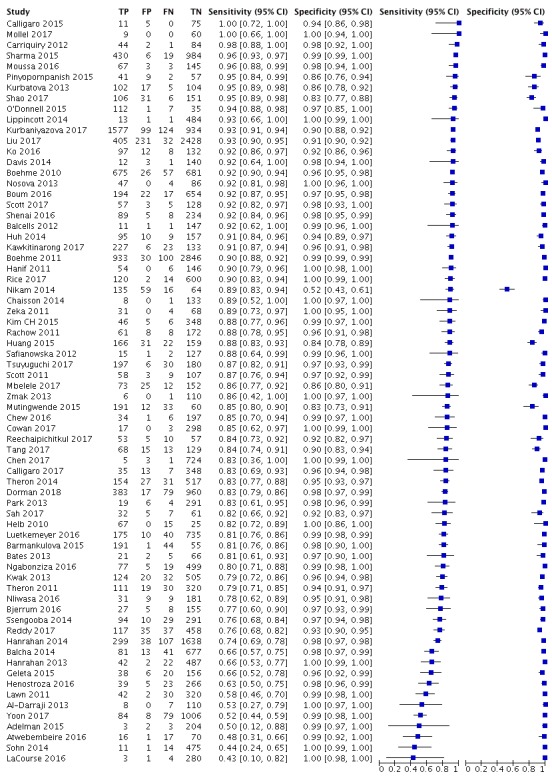
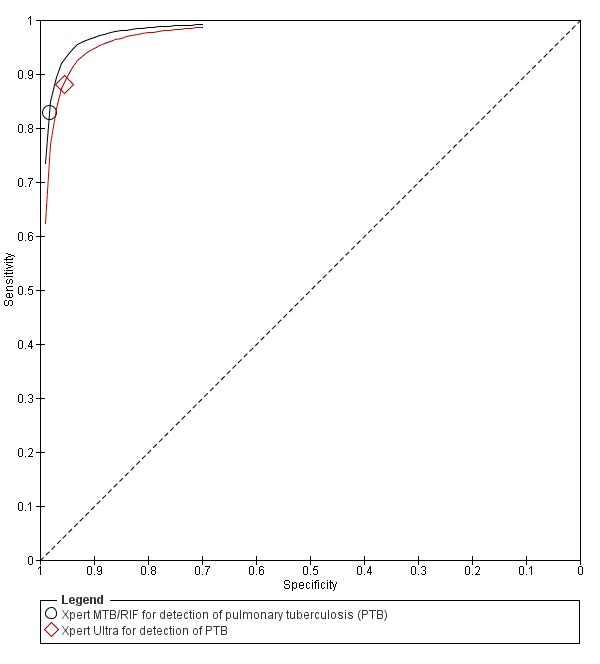
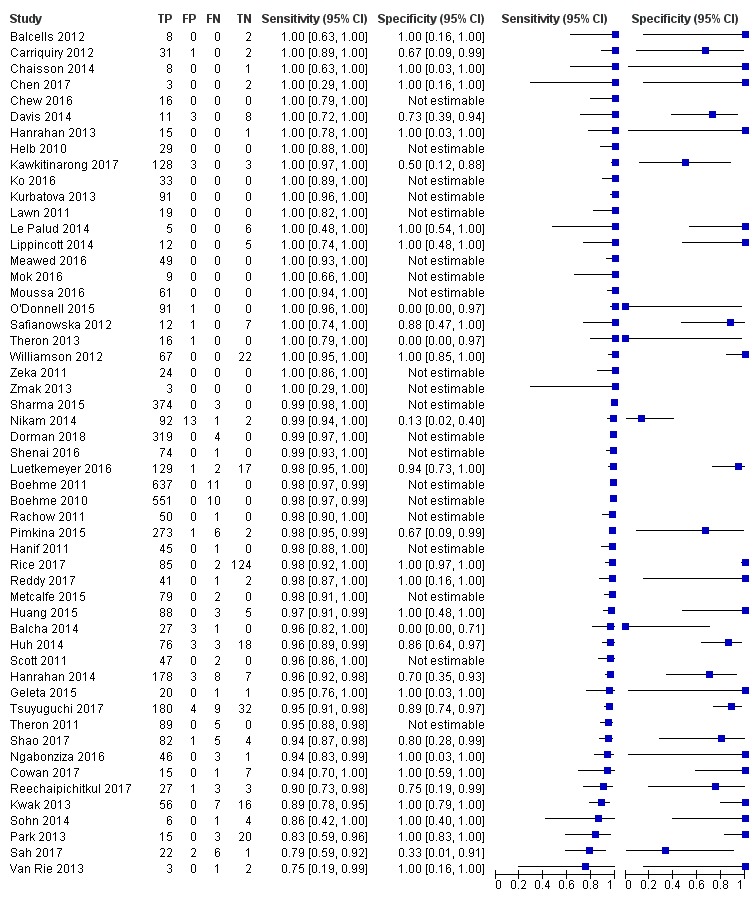
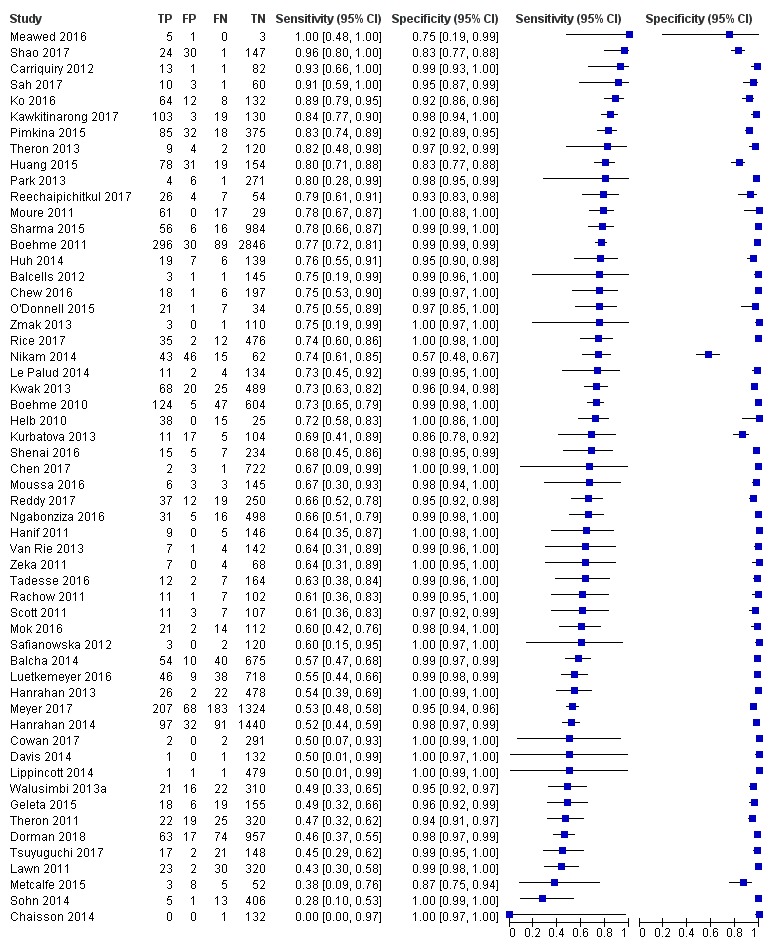
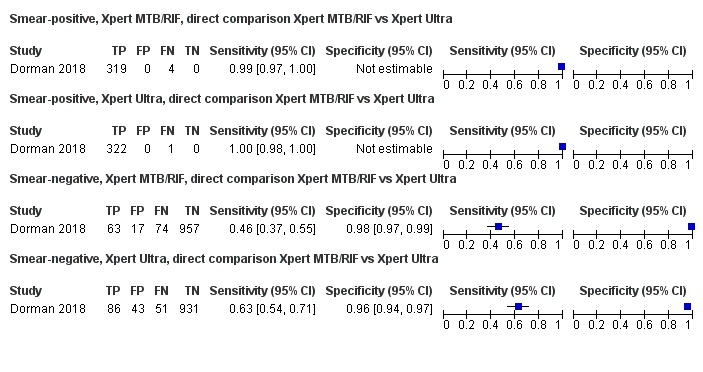
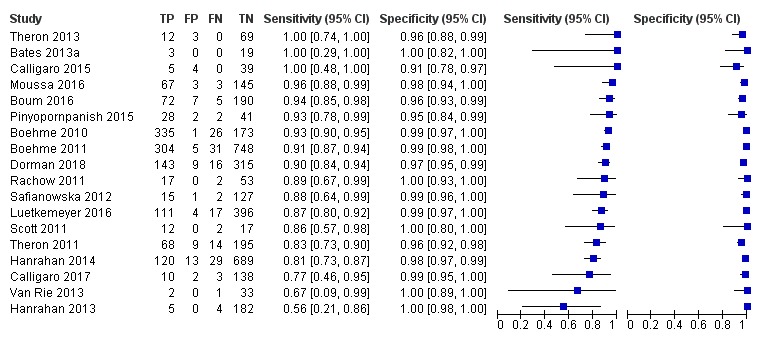
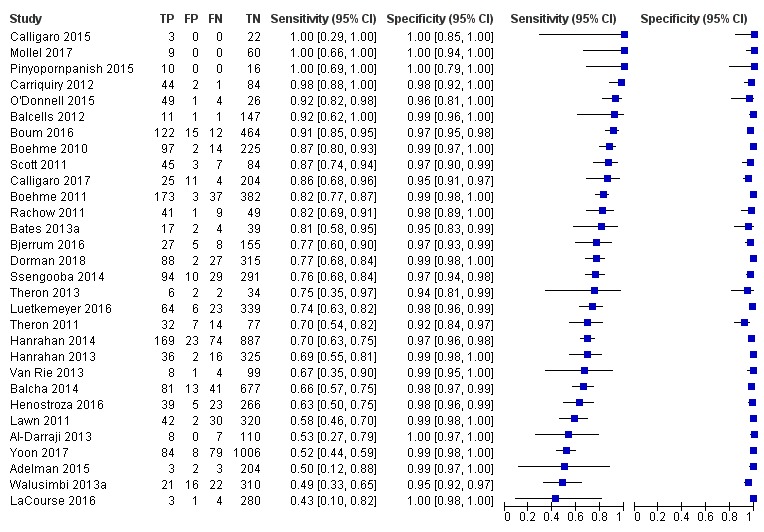
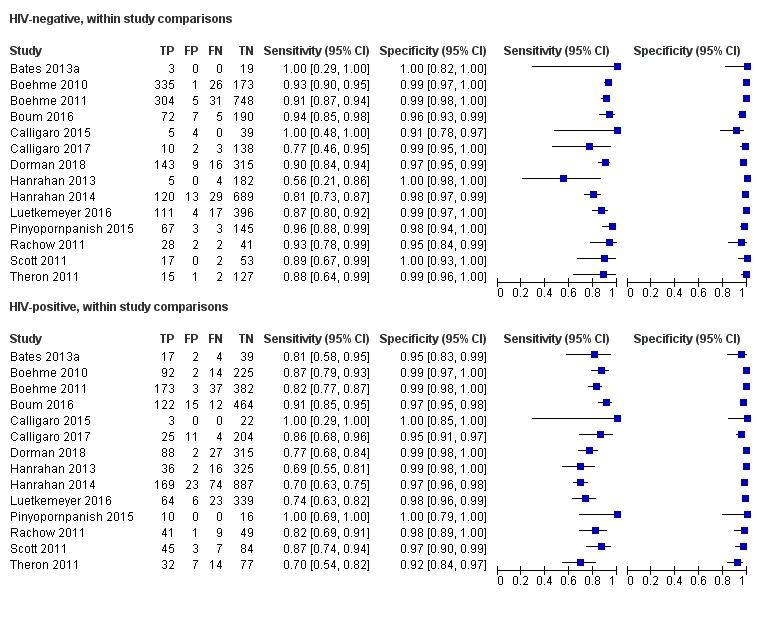
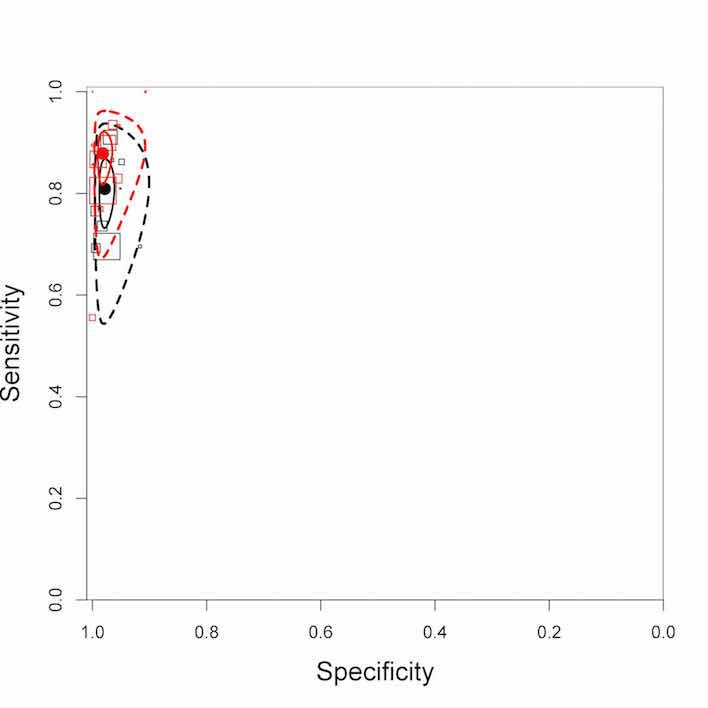
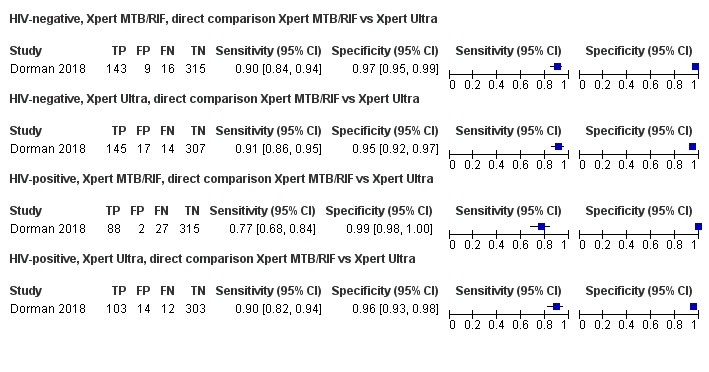
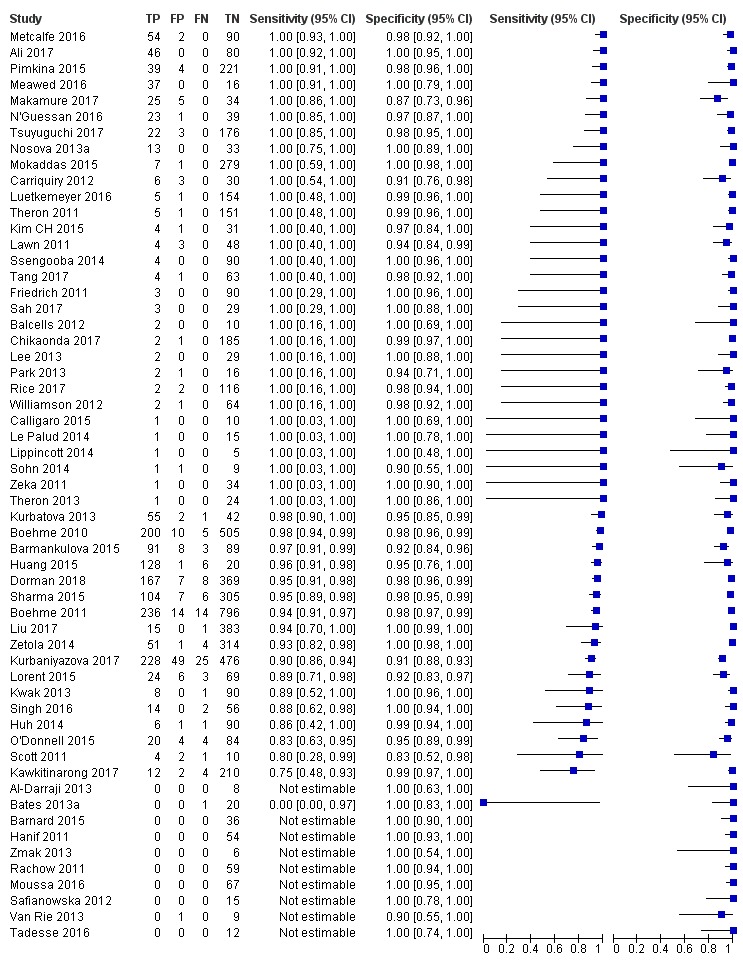
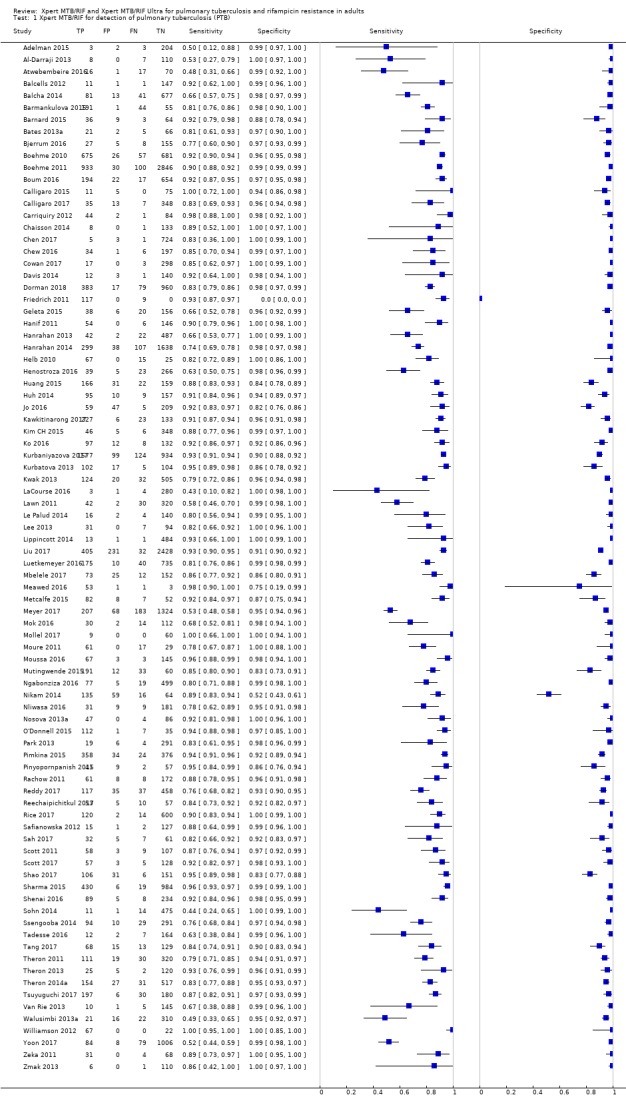
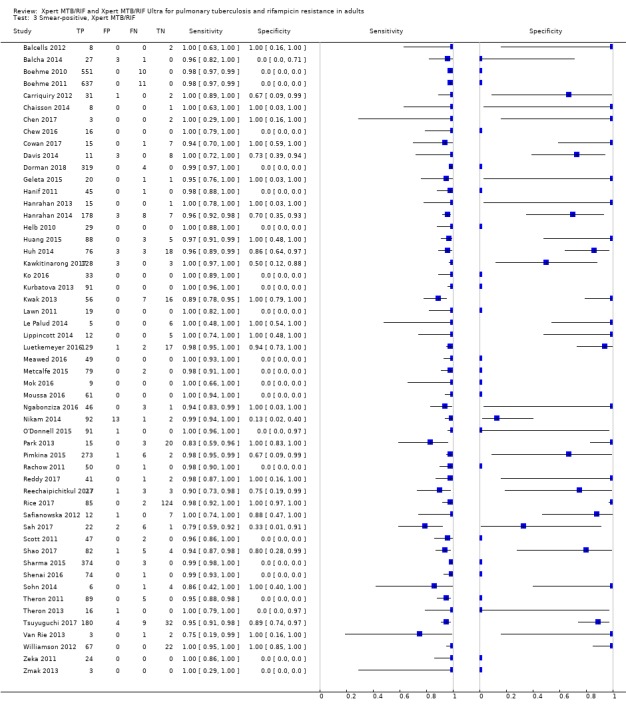
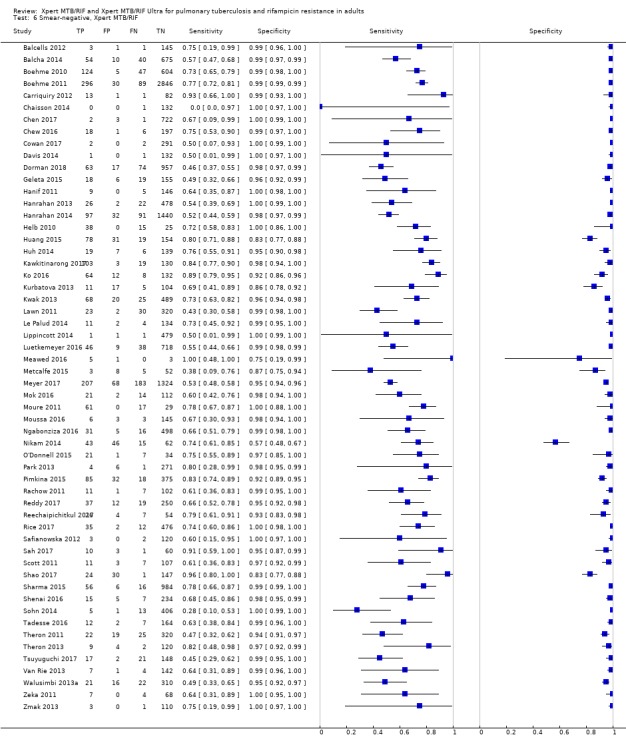
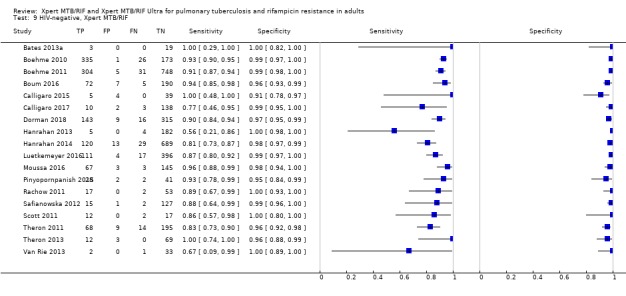
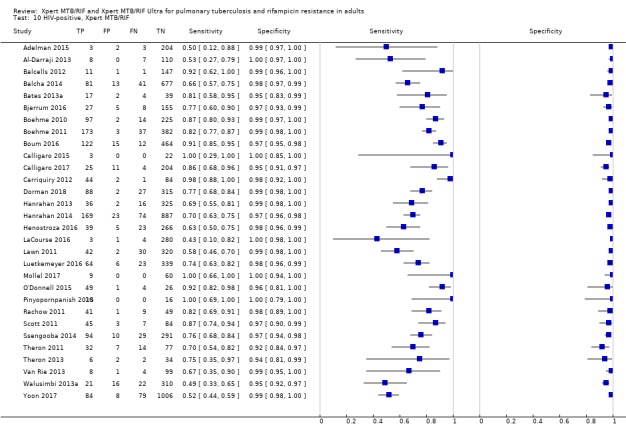
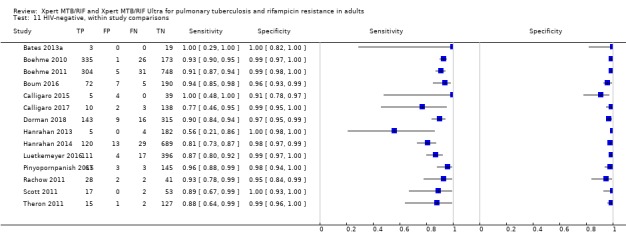
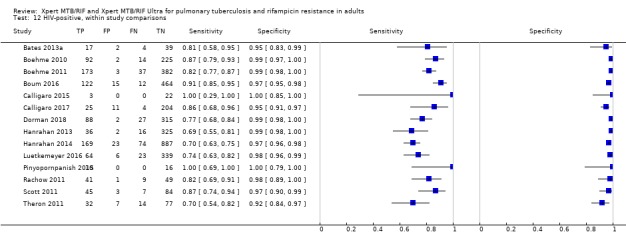
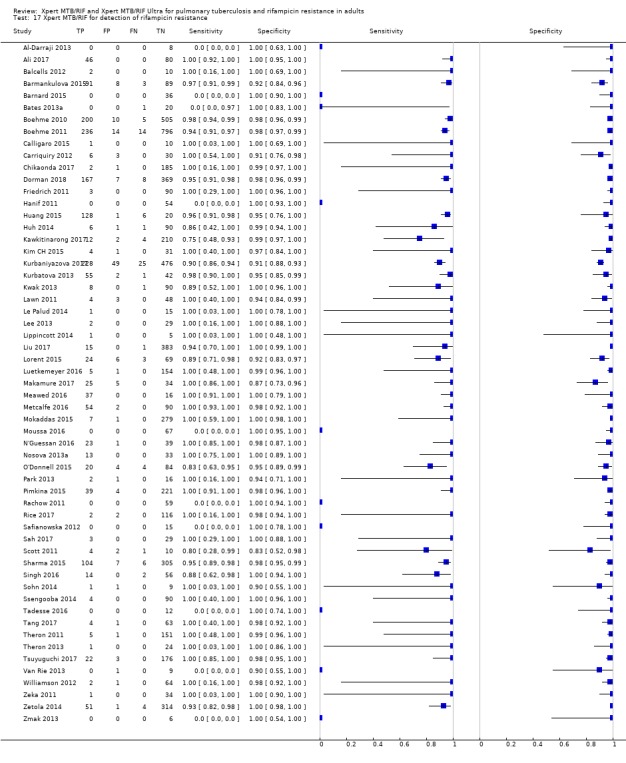
Main results: We identified in total 95 studies (77 new studies since the previous review): 86 studies (42,091 participants) evaluated Xpert MTB/RIF for tuberculosis and 57 studies (8287 participants) for rifampicin resistance. One study compared Xpert MTB/RIF and Xpert Ultra on the same participant specimen.Tuberculosis detectionOf the total 86 studies, 45 took place in high tuberculosis burden and 50 in high TB/HIV burden countries. Most studies had low risk of bias.Xpert MTB/RIF pooled sensitivity and specificity (95% credible Interval (CrI)) were 85% (82% to 88%) and 98% (97% to 98%), (70 studies, 37,237 unselected participants; high-certainty evidence). We found similar accuracy when we included all studies.For a population of 1000 people where 100 have tuberculosis on culture, 103 would be Xpert MTB/RIF-positive and 18 (17%) would not have tuberculosis (false-positives); 897 would be Xpert MTB/RIF-negative and 15 (2%) would have tuberculosis (false-negatives).Xpert Ultra sensitivity (95% confidence interval (CI)) was 88% (85% to 91%) versus Xpert MTB/RIF 83% (79% to 86%); Xpert Ultra specificity was 96% (94% to 97%) versus Xpert MTB/RIF 98% (97% to 99%), (1 study, 1439 participants; moderate-certainty evidence).Xpert MTB/RIF pooled sensitivity was 98% (97% to 98%) in smear-positive and 67% (62% to 72%) in smear-negative, culture-positive participants, (45 studies). Xpert MTB/RIF pooled sensitivity was 88% (83% to 92%) in HIV-negative and 81% (75% to 86%) in HIV-positive participants; specificities were similar 98% (97% to 99%), (14 studies).Rifampicin resistance detectionXpert MTB/RIF pooled sensitivity and specificity (95% Crl) were 96% (94% to 97%) and 98% (98% to 99%), (48 studies, 8020 participants; high-certainty evidence).For a population of 1000 people where 100 have rifampicin-resistant tuberculosis, 114 would be positive for rifampicin-resistant tuberculosis and 18 (16%) would not have rifampicin resistance (false-positives); 886 would be would be negative for rifampicin-resistant tuberculosis and four (0.4%) would have rifampicin resistance (false-negatives).Xpert Ultra sensitivity (95% CI) was 95% (90% to 98%) versus Xpert MTB/RIF 95% (91% to 98%); Xpert Ultra specificity was 98% (97% to 99%) versus Xpert MTB/RIF 98% (96% to 99%), (1 study, 551 participants; moderate-certainty evidence).
Authors' conclusions: We found Xpert MTB/RIF to be sensitive and specific for diagnosing PTB and rifampicin resistance, consistent with findings reported previously. Xpert MTB/RIF was more sensitive for tuberculosis in smear-positive than smear-negative participants and HIV-negative than HIV-positive participants. Compared with Xpert MTB/RIF, Xpert Ultra had higher sensitivity and lower specificity for tuberculosis and similar sensitivity and specificity for rifampicin resistance (1 study). Xpert MTB/RIF and Xpert Ultra provide accurate results and can allow rapid initiation of treatment for multidrug-resistant tuberculosis.
Conflict of interest statement
DJH received financial support for the submitted work from McGill University.
MK has no known conflicts of interest.
JSZ has no known conflicts of interest.
IS has no known conflicts of interest.
ND has no known conflicts of interest.
DT has no known conflicts of interest.
SGS is employed by the Foundation for Innovative New Diagnostics (FIND). FIND has conducted studies and published on Xpert MTB/RIF as part of a collaborative project between FIND, a Swiss non‐profit, Cepheid, a US company, and academic partners. The product developed through this partnership was developed under a contract that obligated FIND to pay for development costs and trial costs and Cepheid to make the test available at specified preferential pricing to the public sector in low‐ and middle‐income countries. In addition, FIND conducted studies for the Xpert MTB/Rif Ultra assay, which have also been published.
EAC has no known conflicts of interest.
MP serves on the Scientific Advisory Committee of FIND, Geneva. FIND is a non‐profit agency that works on global health diagnostics.
KRS received financial support for the submitted work from McGill University, and has received financial support for the preparation of systematic reviews and educational materials, consultancy fees from FIND (for the preparation of systematic reviews), honoraria, and travel support to attend WHO guideline meetings.
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the review apart from those disclosed.
Figures













Update of
-
Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults.Cochrane Database Syst Rev. 2014 Jan 21;2014(1):CD009593. doi: 10.1002/14651858.CD009593.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2019 Jun 07;6:CD009593. doi: 10.1002/14651858.CD009593.pub4. PMID: 24448973 Free PMC article. Updated.
References
References to studies included in this review
-
- Ali RH, Ibrahim NY, Elegail AM, Eltohami NA, Ebraheem RS, Ahmed SF, et al. Evaluation of GeneXpert MTB/RIF and line probe assay for rapid diagnosis of Mycobacterium tuberculosis in Sudanese pulmonary TB patients. Asian Pacific Journal of Tropical Disease 2017;7(7):426‐9.
-
- Atwebembeire J, Orikiriza P, Bonnet M, Atwine D, Katawera V, Nansumba M, et al. Xpert® MTB/RIF for detection of Mycobacterium tuberculosis from frozen string and induced sputum sediments. International Journal of Tuberculosis and Lung Disease 2016;20(8):1113‐7. - PubMed
-
- Balcells ME, García P, Chanqueo L, Bahamondes L, Lasso M, Gallardo AM, et al. Rapid molecular detection of pulmonary tuberculosis in HIV‐infected patients in Santiago, Chile. International Journal of Tuberculosis and Lung Disease 2012;16(10):1349‐53. - PubMed
References to studies excluded from this review
-
- Acuna‐Villaorduna C, Orikiriza P, Nyehangane D, White LF, Mwanga‐Amumpaire J, Kim S, et al. Effect of previous treatment and sputum quality on diagnostic accuracy of Xpert® MTB/RIF. International Journal of Tuberculosis and Lung Disease 2017;21(4):389‐97. - PubMed
-
- Adelman MW, Tsegaye M, Kempker R, Abeje T, Tesfaye A, Aseffa A, et al. Enhanced active TB case finding among people living with hiv: impact of a rapid molecular test (XPERT MTB/RIF). Journal of Investigative Medicine 2014;62(2):570.
-
- Agizew T, Basotli J, Alexander H, Boyd R, Letsibogo G, Auld A, et al. Higher‐than‐expected prevalence of non‐tuberculous mycobacteria in HIV setting in Botswana: implications for diagnostic algorithms using Xpert MTB/RIF assay. PLoS One 2017;12(12):e0189981. [DOI: 10.1371/journal.pone.0189981] - DOI - PMC - PubMed
References to ongoing studies
-
- A trial of same‐day testing and treatment to improve outcomes among symptomatic patients newly diagnosed with HIV. Ongoing study 16 May 2017.
-
- Achieving tuberculosis control In Zambia. Ongoing study 13 April 2018.
-
- Improving tuberculosis diagnosis and treatment through Basic, Applied and health systems Research (BAR). Ongoing study 29 November 2017.
-
- Xpert Ultra and Xpert HIV‐VL in people living with HIV (UltraHIV). Ongoing study 15 June 2017.
-
- Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous bronchoalveolar lavage fluid in HIV‐infected adults: a prospective cohort study. Ongoing study 12 February 2018. - PMC - PubMed
Additional references
-
- American Thoracic Society, the Centers for Disease Control and Prevention, Infectious Disease Society of America. Diagnostic Standards and Classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS Board of Directors, July 1999. This statement was endorsed by the Council of the Infectious Disease Society of America, September 1999. American Journal Respiratory and Critical Care Medicine 2000;161(4 Pt 1):1376‐95. - PubMed
-
- Auld AF, Fielding KL, Gupta‐Wright A, Lawn SD. Xpert MTB/RIF ‐ why the lack of morbidity and mortality impact in intervention trials?. Transactions of the Royal Society of Tropical Medicine and Hygiene 2016;110(8):432‐44. - PubMed
-
- Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. Journal of Clinical Epidemiology 2011;64(4):401‐6. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources