

Minor salivary gland tumors of the head and neck-Memorial Sloan Kettering experience: Incidence and outcomes by site and histological type
- PMID: 31174233
- PMCID: PMC6744325
- DOI: 10.1002/cncr.32208
Minor salivary gland tumors of the head and neck-Memorial Sloan Kettering experience: Incidence and outcomes by site and histological type
Abstract
Background: Minor salivary gland carcinomas of the head and neck are rare cancers with variable clinical behavior. This study explored the incidence, pathology, clinical behavior, and factors predictive of outcomes in a large cohort of patients treated at Memorial Sloan Kettering Cancer Center over a 30-year period (1985-2015).
Methods: Clinical, pathological, treatment, and outcome data were collected. Unadjusted and adjusted hazard ratios for each variable were calculated with univariate and multivariable Cox regression for survival and recurrence outcomes.
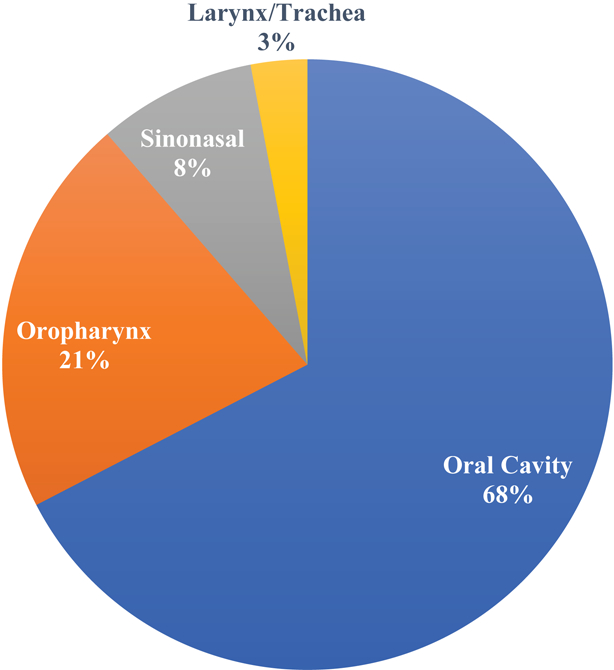
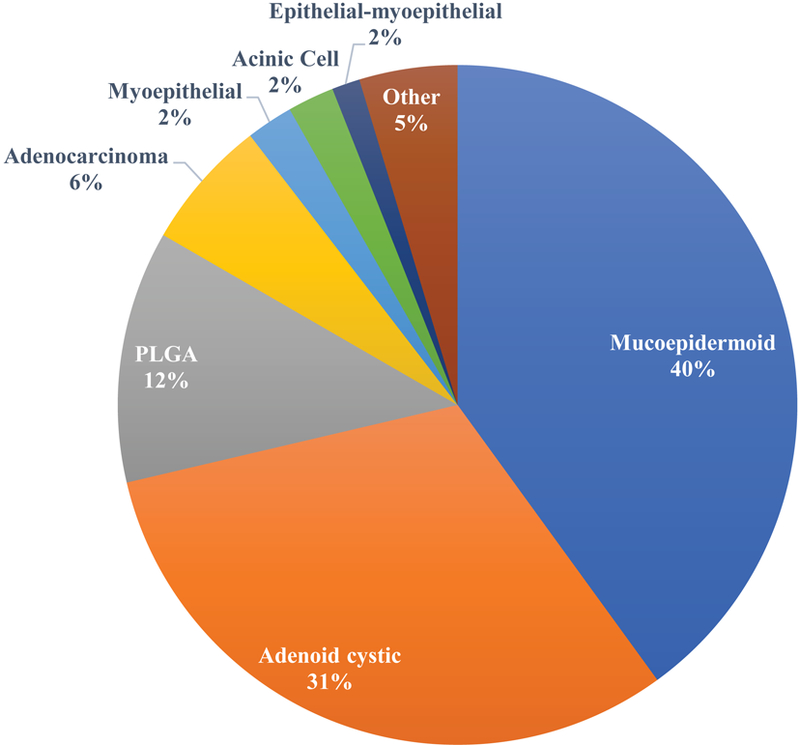
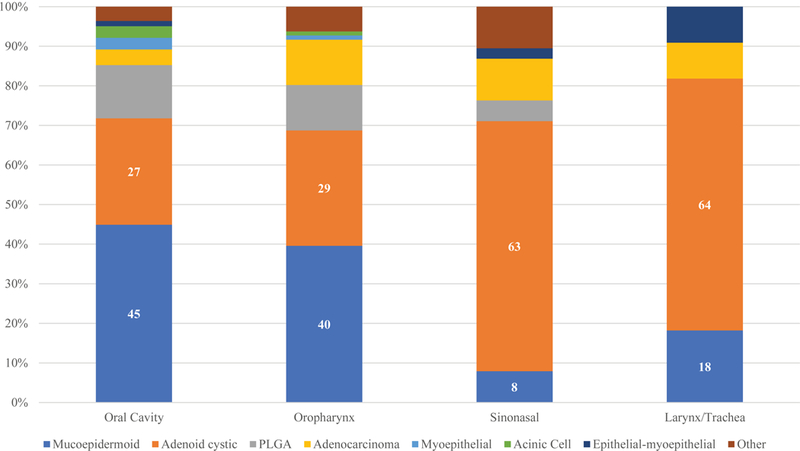
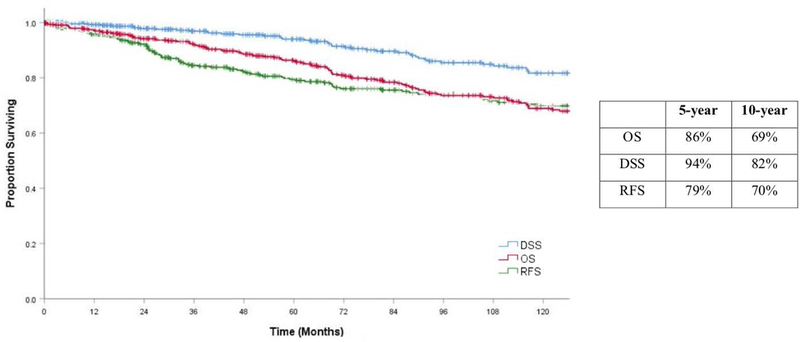
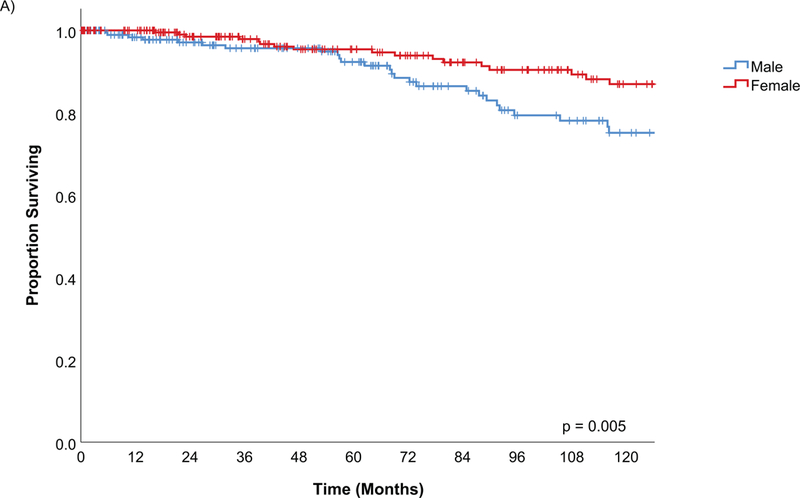
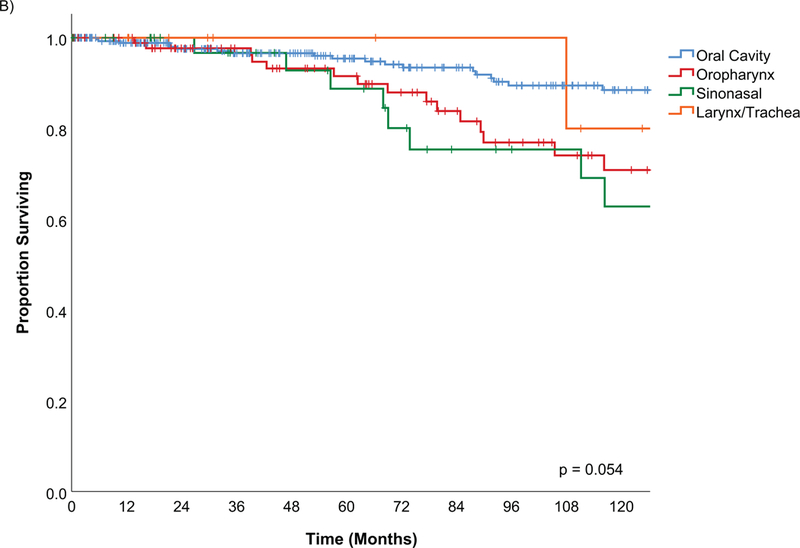
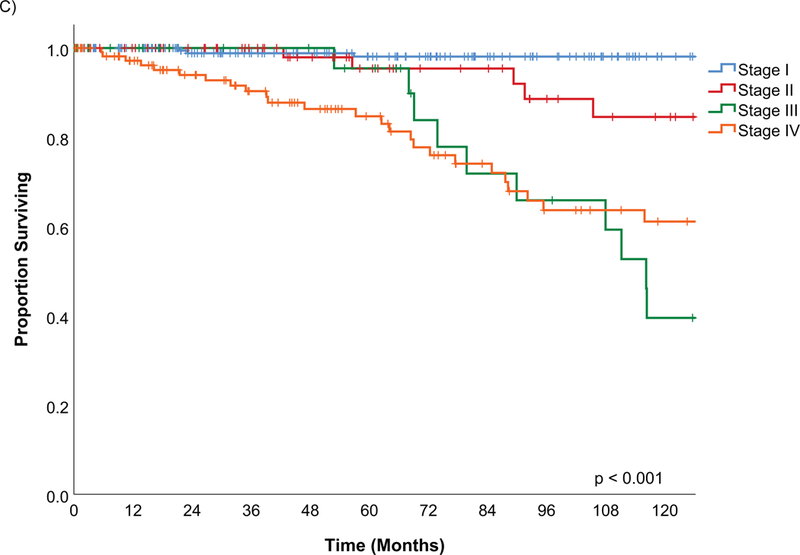
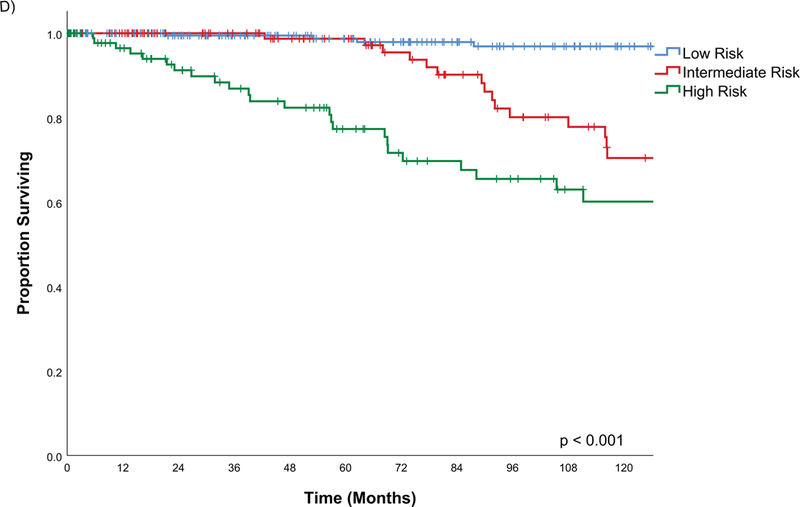
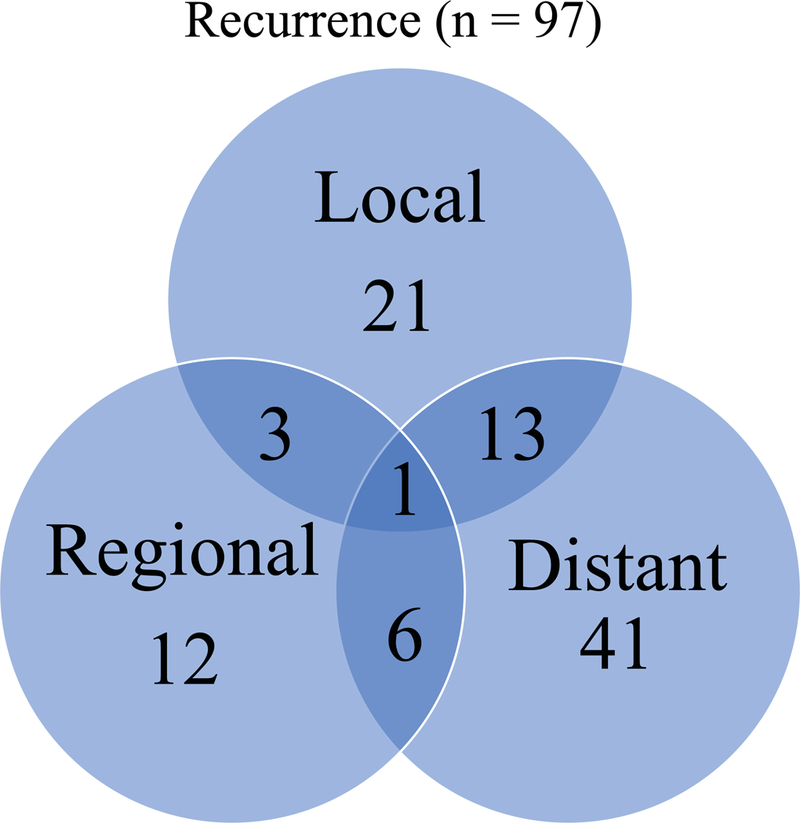
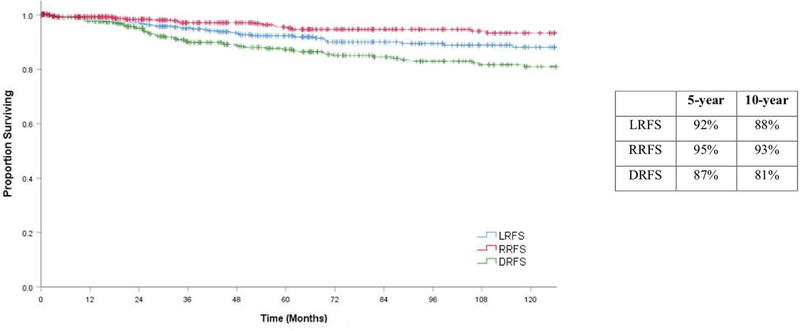
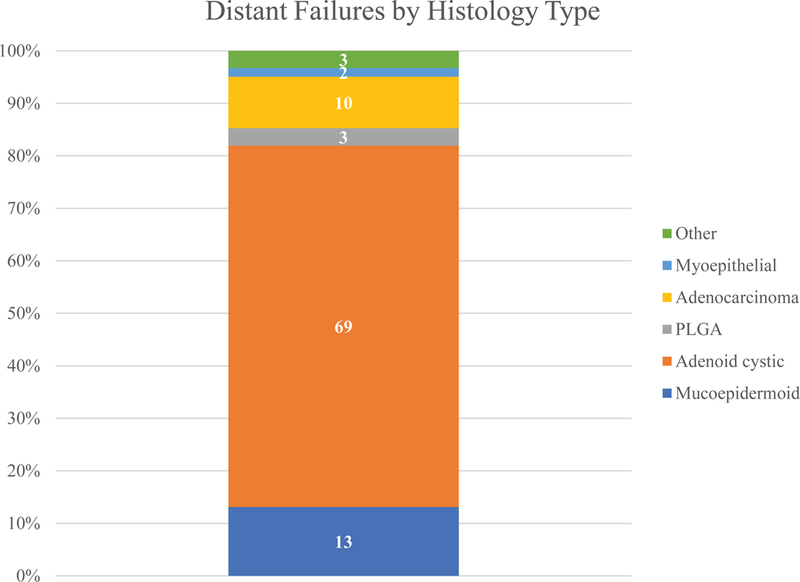
Results: Four hundred fifty patients were included: 55% were female, 56% were younger than 60 years, and the median follow-up was 74 months (range, 1-364 months). The most common site was the oral cavity with 305 tumors (68%), which was followed by the oropharynx with 96 (21%), the sinonasal cavity with 38 (8%), the trachea with 7 (2%), and the larynx with 4 (1%). The most common histological types were mucoepidermoid carcinoma (180 tumors [40%]), adenoid cystic carcinoma (141 tumors [31%]), and polymorphous low-grade adenocarcinoma (54 tumors [12%]). The 5-year predicted overall survival rate was 86%, and the disease-specific survival rate was 94% at 5 years. Pathology and tumor stage were significant variables on multivariate analysis for overall survival, disease-specific survival, recurrence-free survival, local recurrence-free survival, regional recurrence-free survival, and distant recurrence-free survival.
Conclusions: American Joint Committee on Cancer stage and pathology were the most predictive variables across all outcomes. Tumor site, postoperative radiotherapy, and margin status were not statistically significant variables after tumor stage and pathology were controlled for in most outcomes.
Keywords: head and neck cancer; minor salivary gland carcinoma; outcomes; prediction; survival.
© 2019 American Cancer Society.
Conflict of interest statement
Figures
References
-
- Albeck H, Nielsen NH, Hansen HE, Bentzen J, Ockelmann HH, Bretlau P, et al. Epidemiology of nasopharyngeal and salivary gland carcinoma in Greenland. Arctic Med Res 1992;51(4):189–95. - PubMed
-
- Vander Poorten V, Hunt J, Bradley PJ, Haigentz M Jr., Rinaldo A, Mendenhall WM, et al. Recent trends in the management of minor salivary gland carcinoma. Head Neck 2014;36(3):444–55. - PubMed
-
- Bradley PJ, McGurk M. Incidence of salivary gland neoplasms in a defined UK population. Br J Oral Maxillofac Surg 2013;51(5):399–403. - PubMed
-
- Myers EN, Ferris RL. Salivary gland disorders Berlin; [London]: Springer; 2007. xv, 517 p. : ill. (chiefly col.); 25 cm. p.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
