

Decompressive craniectomy for acute ischemic stroke
- PMID: 31174580
- PMCID: PMC6556035
- DOI: 10.1186/s13054-019-2490-x
Decompressive craniectomy for acute ischemic stroke
Abstract
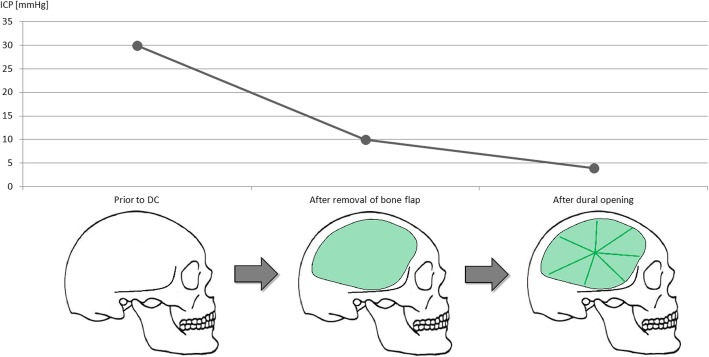
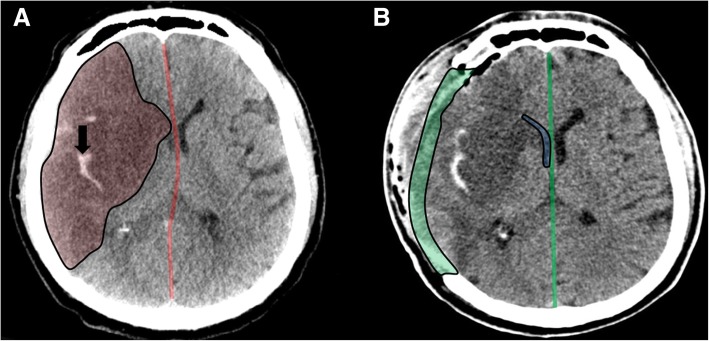
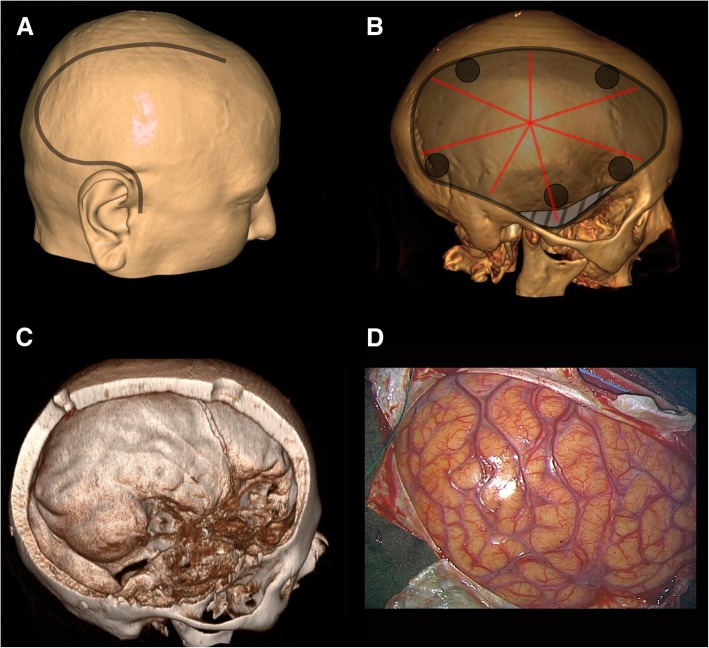
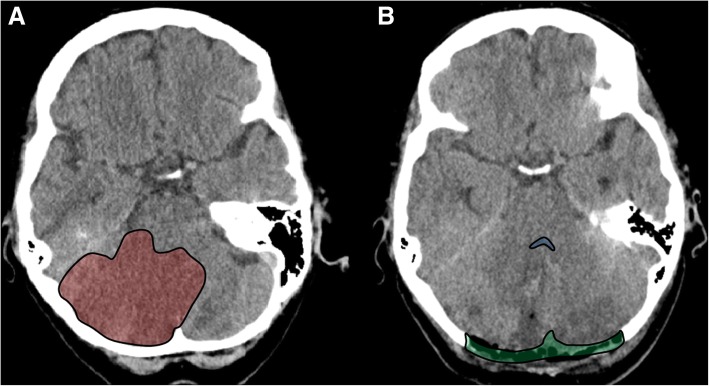
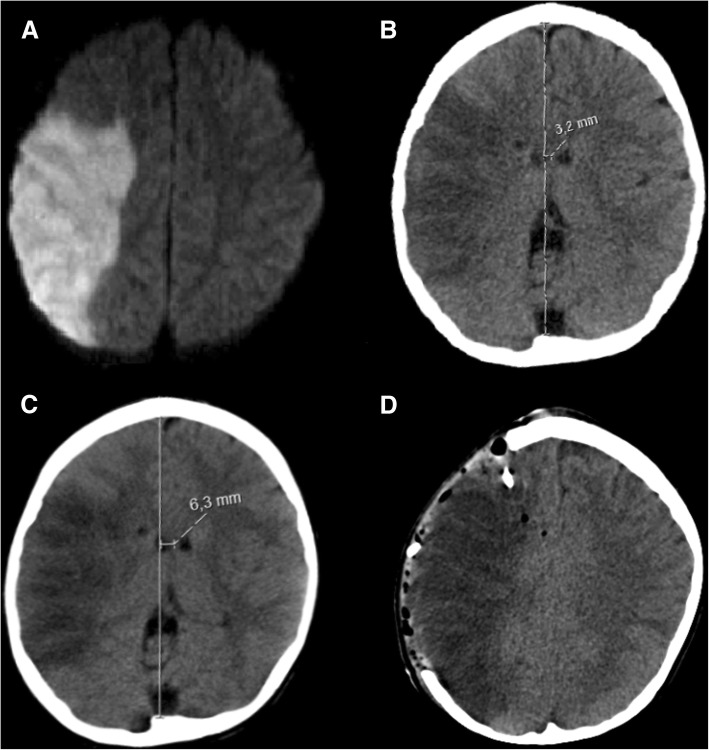
Malignant stroke occurs in a subgroup of patients suffering from ischemic cerebral infarction and is characterized by neurological deterioration due to progressive edema, raised intracranial pressure, and cerebral herniation. Decompressive craniectomy (DC) is a surgical technique aiming to open the "closed box" represented by the non-expandable skull in cases of refractory intracranial hypertension. It is a valuable modality in the armamentarium to treat patients with malignant stroke: the life-saving effect has been proven for both supratentorial and infratentorial DC in virtually all age groups. This leaves physicians with the difficult task to decide who will require early or preemptive surgery and who might benefit from postponing surgery until clear evidence of deterioration evolves. Together with the patient's relatives, physicians also have to ascertain whether the patient will have acceptable disability and quality of life in his or her presumed perception, based on preoperative predictions. This complex decision-making process can only be managed with interdisciplinary efforts and should be supported by continued research in the age of personalized medicine.
Keywords: Cranioplasty; Decompressive craniectomy; Hemicraniectomy; Malignant ischemic infarction; Pediatric stroke; Suboccipital craniectomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Kocher T. Hirnerschütterung, Hirndruck und chirurgische Eingriffe bei Hirnkrankheiten. Wien: Alfred Hölder; 1901.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
