

Neuroimaging correlates with neuropathologic schemes in neurodegenerative disease
- PMID: 31175025
- PMCID: PMC6662599
- DOI: 10.1016/j.jalz.2019.03.016
Neuroimaging correlates with neuropathologic schemes in neurodegenerative disease
Abstract
Introduction: Neuroimaging biomarkers are important for early diagnosis of Alzheimer's disease, and comparing multimodality neuroimaging to autopsy data is essential.
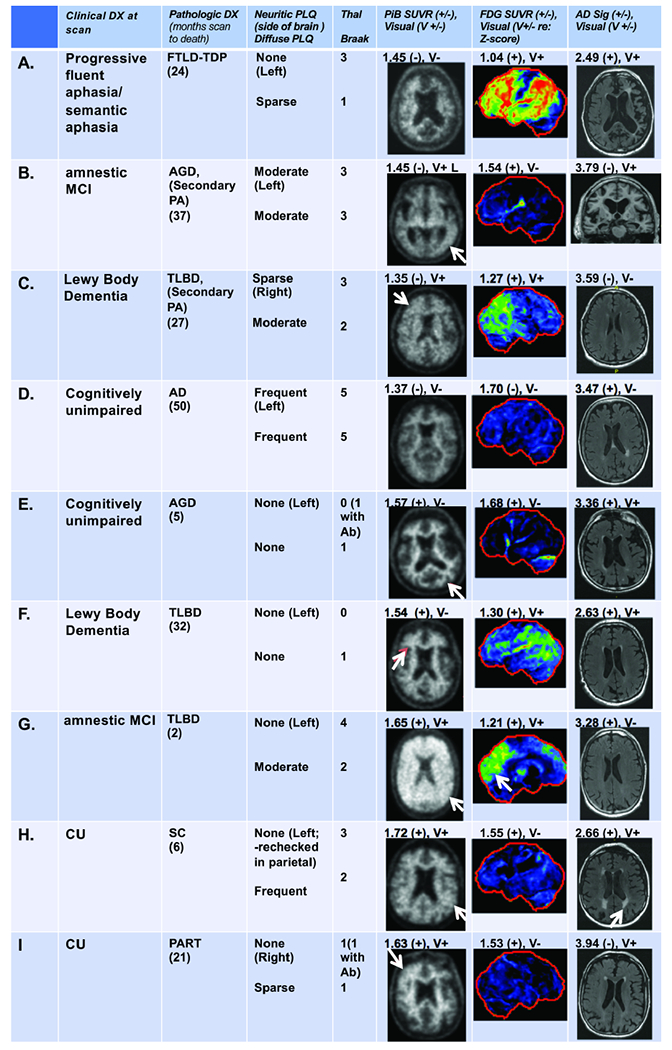
Methods: We compared the pathologic findings from a prospective autopsy cohort (n = 100) to Pittsburgh compound B PET (PiB-PET), 18F-fluorodeoxyglucose PET (FDG-PET), and MRI. Correlations between neuroimaging biomarkers and neuropathologic schemes were assessed.
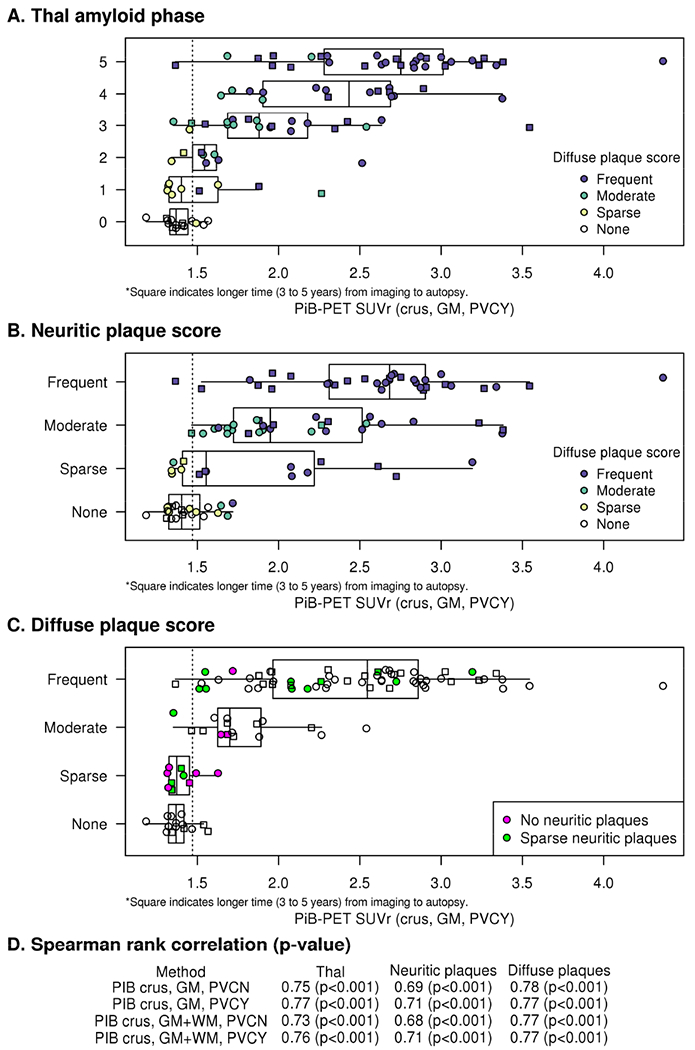
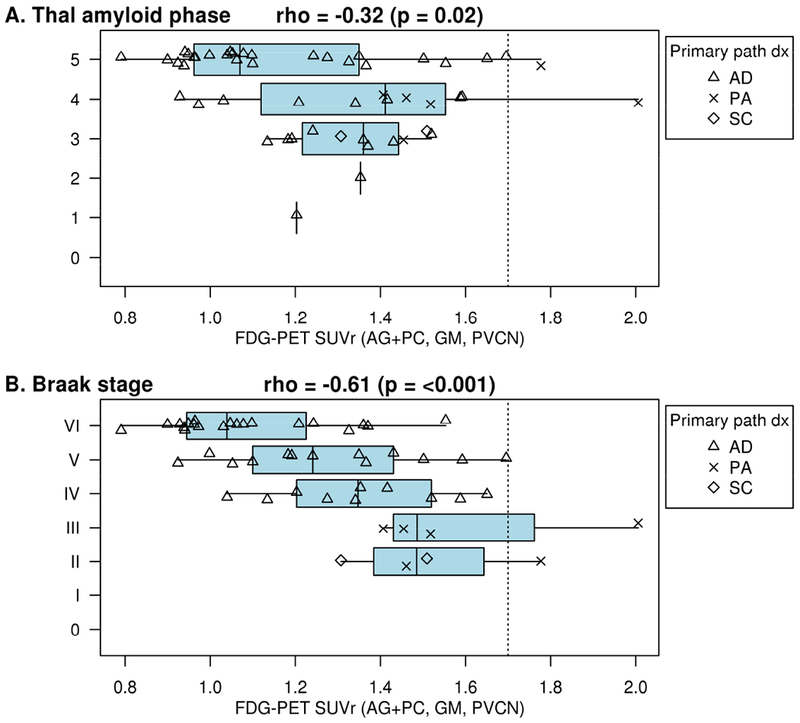
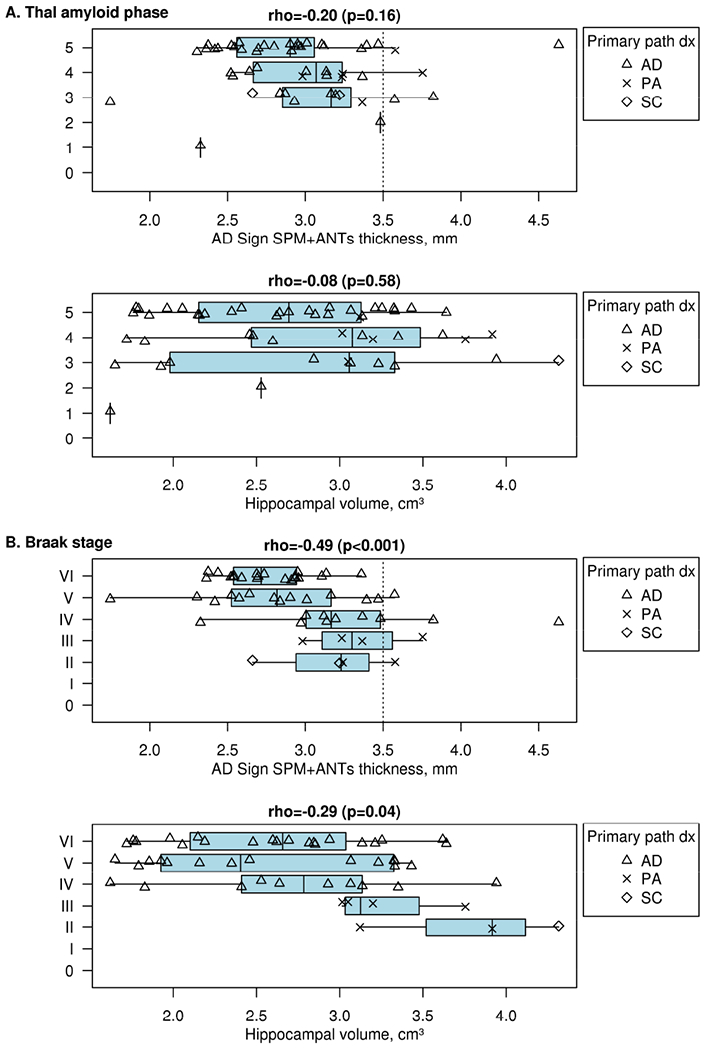
Results: PiB-PET showed strong correlations with Thal amyloid phase and Consortium to Establish a Registry for Alzheimer's Disease score and categorized 44% of Thal phase 1 participants as positive. FDG-PET and MRI correlated modestly with Braak tangle stage in Alzheimer's type pathology. A subset of participants with "none" or "sparse" neuritic plaque scores had elevated PiB-PET signal due to diffuse amyloid plaque. Participants with findings characterized as "suspected non-Alzheimer's pathophysiology" represented 15% of the group.
Discussion: PiB-PET is associated with Alzheimer's disease, neuritic plaques, and diffuse plaques. FDG-PET and MRI have modest correlation with neuropathologic schemes. Participants with findings characterized as suspected non-Alzheimer's pathophysiology most commonly had primary age-related tauopathy.
Keywords: Alzheimer's disease; Amyloid; Amyloid-PET; Autopsy; Braak tangle stage; CERAD; Dementia; MRI; Mild cognitive impairment; Neurodegeneration; SNAP; Tau-PET; Thal amyloid stage.
Copyright © 2019 the Alzheimer's Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Clark CM, Pontecorvo MJ, Beach TG, Bedell BJ, Coleman RE, Doraiswamy PM, et al. Cerebral PET with florbetapir compared with neuropathology at autopsy for detection of neuritic amyloid-beta plaques: a prospective cohort study. Lancet neurology. 2012;11:669–78. - PubMed
-
- Johnson KA, Gregas M, Becker JA, Kinnecom C, Salat DH, Moran EK, et al. Imaging of amyloid burden and distribution in cerebral amyloid angiopathy. Ann Neurol. 2007;62:229–34. - PubMed
-
- Klunk WE, Engler H, Nordberg A, Wang Y, Blomqvist G, Holt DP, et al. Imaging brain amyloid in Alzheimer’s disease with Pittsburgh Compound-B. Annals of Neurology. 2004;55:306–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG041851/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- R01 AG054449/AG/NIA NIH HHS/United States
- R01 AG011378/AG/NIA NIH HHS/United States
- RF1 AG057547/AG/NIA NIH HHS/United States
- P30 AG062677/AG/NIA NIH HHS/United States
- R37 AG011378/AG/NIA NIH HHS/United States
- R01 NS089544/NS/NINDS NIH HHS/United States
- U01 NS100620/NS/NINDS NIH HHS/United States
- U01 AG006786/AG/NIA NIH HHS/United States
- R01 AG040042/AG/NIA NIH HHS/United States
- R21 NS094489/NS/NINDS NIH HHS/United States
- R01 NS089757/NS/NINDS NIH HHS/United States
- R01 DC010367/DC/NIDCD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
