

Prevalence of non-suicidal self-harm and service contact in England, 2000-14: repeated cross-sectional surveys of the general population
- PMID: 31175059
- PMCID: PMC7646286
- DOI: 10.1016/S2215-0366(19)30188-9
Prevalence of non-suicidal self-harm and service contact in England, 2000-14: repeated cross-sectional surveys of the general population
Abstract
Background: The number of people presenting to hospital emergency departments after self-harming has increased in England. However, most people who self-harm do not present to hospitals, so whether this rise reflects an increase in the prevalence of self-harm in the community is unknown. Also unknown is whether the prevalence of non-suicidal self-harm (NSSH) or suicidal self-harm, or both, has increased. We aimed to establish temporal trends in the prevalence of NSSH in England.
Methods: We analysed data from participants in the 2000 (n=7243), 2007 (n=6444), and 2014 (n=6477) Adult Psychiatric Morbidity Surveys of the general population, selecting those aged 16-74 years and living in England. We used weighted data and controlled for complex survey design. We generated temporal trends in lifetime prevalence and methods of, and motivations for, NSSH, and consequent service contact. We used multiple variable logistic regression analyses to investigate factors associated with service contact.
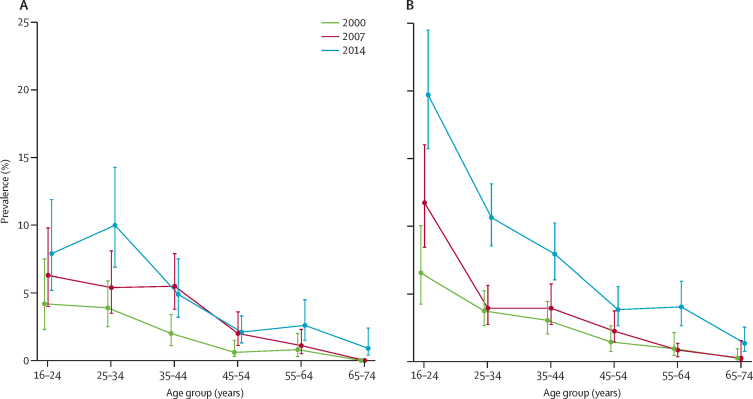
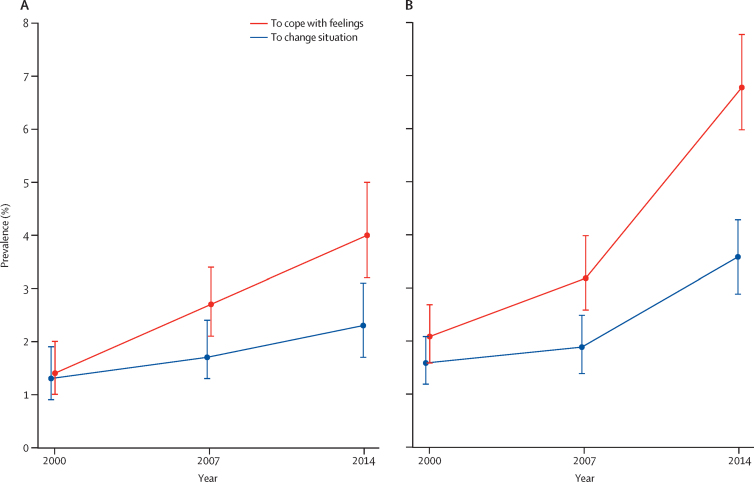
Findings: The prevalence of self-reported lifetime NSSH increased from 2·4% (95% CI 2·0-2·8) in 2000, to 6·4% (5·8-7·2) in 2014. Increases in prevalence were noted in both sexes and across age groups-most notably in women and girls aged 16-24 years, in whom prevalence increased from 6·5% (4·2-10·0) in 2000, to 19·7% (15·7-24·5) in 2014. The proportion of the population reporting NSSH to relieve unpleasant feelings of anger, tension, anxiety, or depression increased from 1·4% (95% CI 1·0-2·0) to 4·0% (3·2-5·0) in men and boys, and from 2·1% (1·6-2·7) to 6·8% (6·0-7·8) in women and girls, between 2000 and 2014. In 2014, 59·4% (95% CI 54·7-63·9) of participants who had engaged in NSSH reported no consequent medical or psychological service contact, compared with 51·2% (42·2-60·0) in 2000 and 51·8% (47·3-56·4) in 2007. Male participants and those aged 16-34 years were less likely to have contact with health services than were female participants and older people.
Interpretation: The prevalence of NSSH has increased in England, but resultant service contact remains low. In 2014, about one in five female 16-24-year-olds reported NSSH. There are potential lifelong implications of NSSH, such as an increased frequency of suicide, especially if the behaviours are adopted as a long-term coping strategy. Self-harm needs to be discussed with young people without normalising it. Young people should be offered help by primary care, educational, and other services to find safer ways to deal with emotional stress.
Funding: NHS Digital, English Department of Health and Social Care, and the National Institute for Health Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Responding to the rising prevalence of self-harm.Lancet Psychiatry. 2019 Jul;6(7):548-549. doi: 10.1016/S2215-0366(19)30210-X. Epub 2019 Jun 4. Lancet Psychiatry. 2019. PMID: 31175058 No abstract available.
-
Supporting young people with self-harm behaviour in primary care.Lancet Psychiatry. 2019 Sep;6(9):724. doi: 10.1016/S2215-0366(19)30280-9. Lancet Psychiatry. 2019. PMID: 31448751 No abstract available.
References
-
- Hawton K, Harriss L, Zahl D. Deaths from all causes in a long-term follow-up study of 11 583 deliberate self-harm patients. Psychol Med. 2006;36:397–405. - PubMed
