

Design and Evaluation of an External Control Arm Using Prior Clinical Trials and Real-World Data
- PMID: 31175098
- PMCID: PMC6697596
- DOI: 10.1158/1078-0432.CCR-19-0820
Design and Evaluation of an External Control Arm Using Prior Clinical Trials and Real-World Data
Abstract
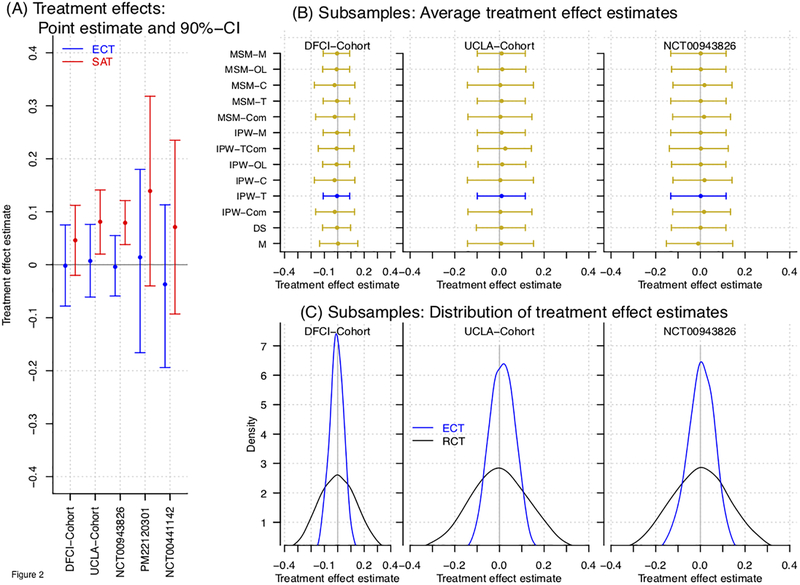
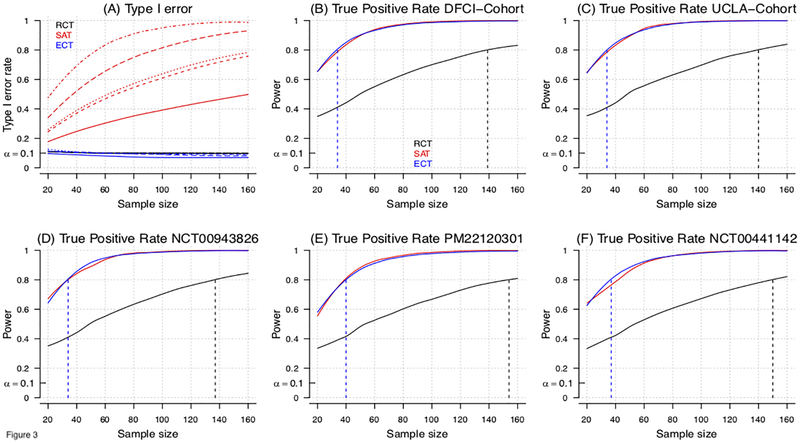
Purpose: We discuss designs and interpretable metrics of bias and statistical efficiency of "externally controlled" trials (ECT) and compare ECT performance to randomized and single-arm designs.
Experimental design: We specify an ECT design that leverages information from real-world data (RWD) and prior clinical trials to reduce bias associated with interstudy variations of the enrolled populations. We then used a collection of clinical studies in glioblastoma (GBM) and RWD from patients treated with the current standard of care to evaluate ECTs. Validation is based on a "leave one out" scheme, with iterative selection of a single-arm from one of the studies, for which we estimate treatment effects using the remaining studies as external control. This produces interpretable and robust estimates on ECT bias and type I errors.
Results: We developed a model-free approach to evaluate ECTs based on collections of clinical trials and RWD. For GBM, we verified that inflated false positive error rates of standard single-arm trials can be considerably reduced (up to 30%) by using external control data.
Conclusions: The use of ECT designs in GBM, with adjustments for the clinical profiles of the enrolled patients, should be preferred to single-arm studies with fixed efficacy thresholds extracted from published results on the current standard of care.
©2019 American Association for Cancer Research.
Figures

References
-
- Marshall G, Blacklock JW, Cameron C, et al. Streptomycin Treatment of Pulmonary Tuberculosis: A Medical Research Council Investigation. Bmj. 1948. doi:10.1136/bmj.2.4582.769 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
