

Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis
- PMID: 31175501
- PMCID: PMC7205855
- DOI: 10.1007/s10877-019-00330-y
Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis
Abstract
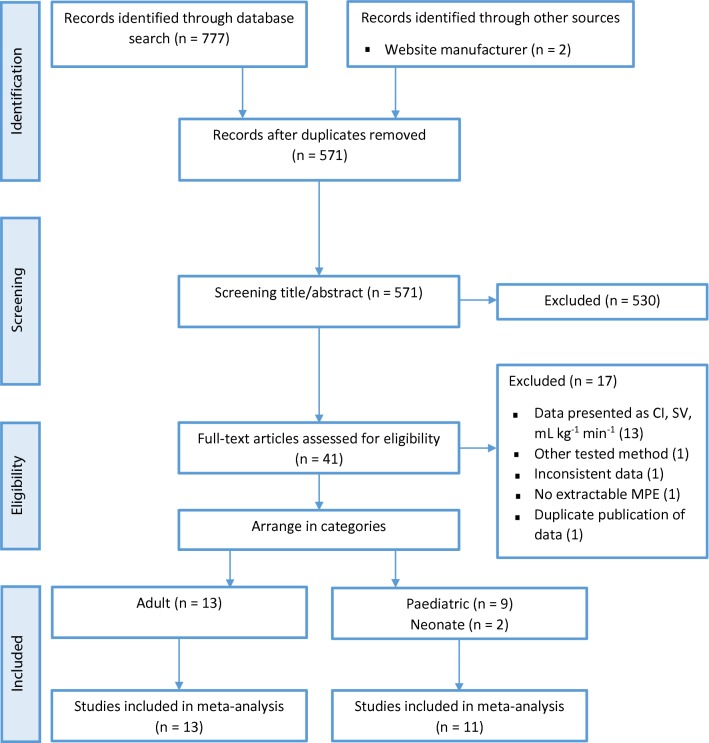
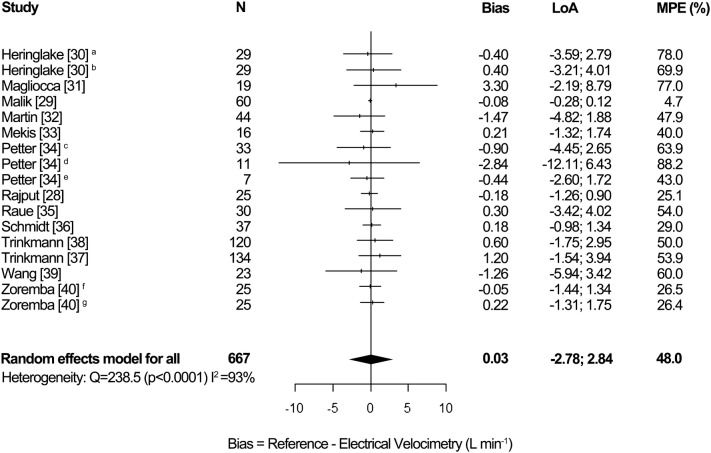
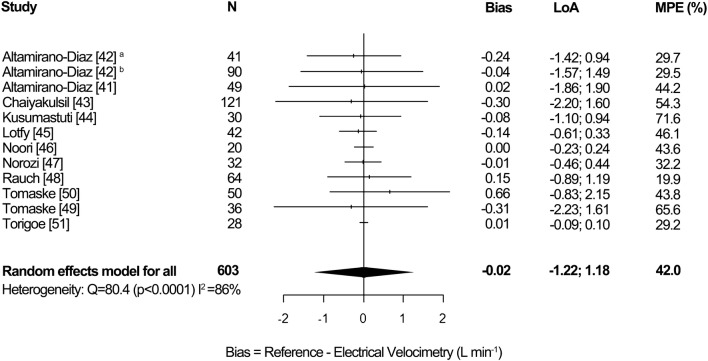
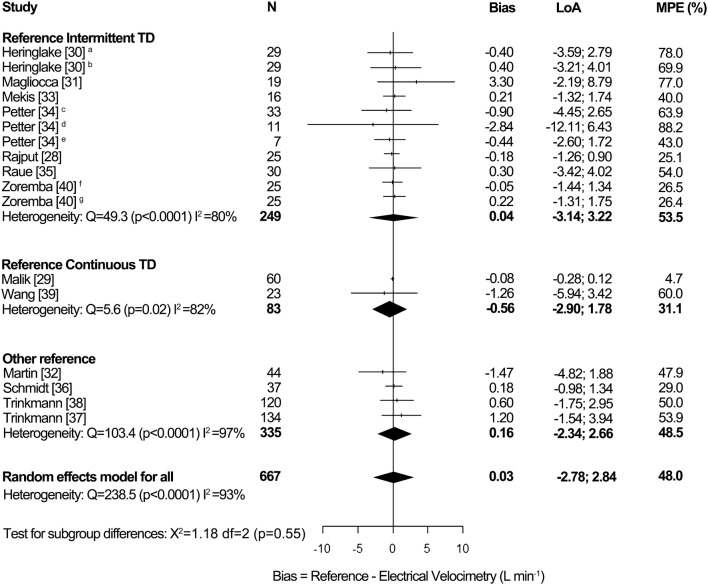
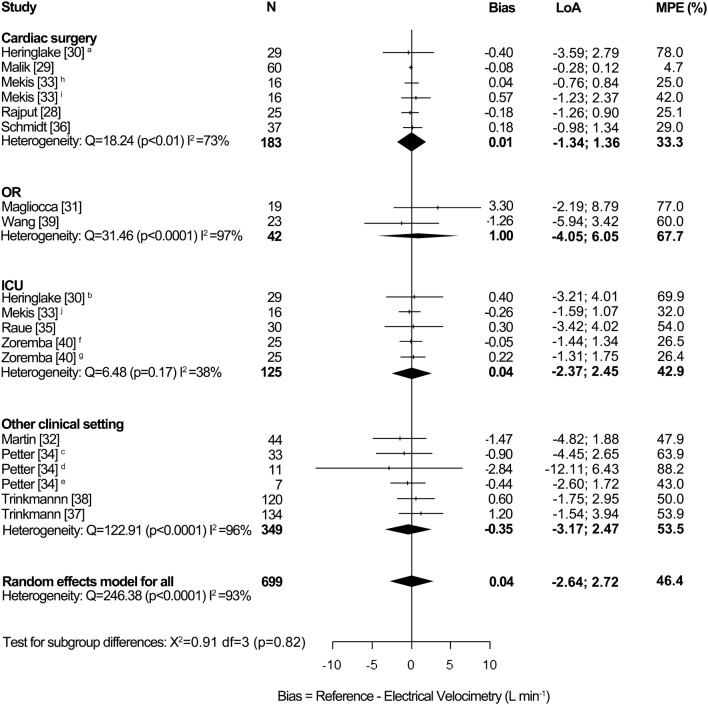
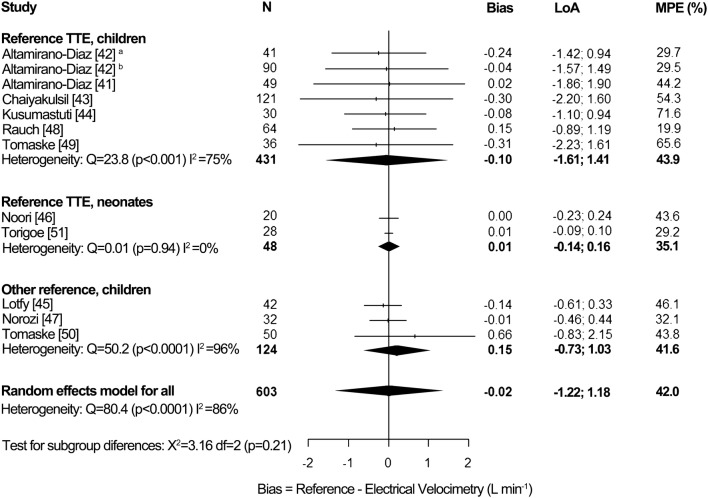
Cardiac output monitoring is used in critically ill and high-risk surgical patients. Intermittent pulmonary artery thermodilution and transpulmonary thermodilution, considered the gold standard, are invasive and linked to complications. Therefore, many non-invasive cardiac output devices have been developed and studied. One of those is electrical cardiometry. The results of validation studies are conflicting, which emphasize the need for definitive validation of accuracy and precision. We performed a database search of PubMed, Embase, Web of Science and the Cochrane Library of Clinical Trials to identify studies comparing cardiac output measurement by electrical cardiometry and a reference method. Pooled bias, limits of agreement (LoA) and mean percentage error (MPE) were calculated using a random-effects model. A pooled MPE of less than 30% was considered clinically acceptable. A total of 13 studies in adults (620 patients) and 11 studies in pediatrics (603 patients) were included. For adults, pooled bias was 0.03 L min-1 [95% CI - 0.23; 0.29], LoA - 2.78 to 2.84 L min-1 and MPE 48.0%. For pediatrics, pooled bias was - 0.02 L min-1 [95% CI - 0.09; 0.05], LoA - 1.22 to 1.18 L min-1 and MPE 42.0%. Inter-study heterogeneity was high for both adults (I2 = 93%, p < 0.0001) and pediatrics (I2 = 86%, p < 0.0001). Despite the low bias for both adults and pediatrics, the MPE was not clinically acceptable. Electrical cardiometry cannot replace thermodilution and transthoracic echocardiography for the measurement of absolute cardiac output values. Future research should explore it's clinical use and indications.
Keywords: Bioimpedance; Cardiac output; Electrical cardiometry; Electrical velocimetry; Hemodynamic monitoring; Meta-analysis; Non-invasive; Systematic review.
Conflict of interest statement
CS contacted the manufacturer of the Aesculon® and ICON® monitor (Osypka Medical GmbH, Berlin, Germany) for identification of additional studies. Besides this, the authors declare that they have no conflict of interest.
Figures
Similar articles
-
Electrical cardiometry for non-invasive cardiac output monitoring: a method comparison study in patients after coronary artery bypass graft surgery.J Clin Monit Comput. 2025 Apr;39(2):371-376. doi: 10.1007/s10877-024-01246-y. Epub 2024 Dec 11. J Clin Monit Comput. 2025. PMID: 39661264 Free PMC article.
-
Agreement between continuous and intermittent pulmonary artery thermodilution for cardiac output measurement in perioperative and intensive care medicine: a systematic review and meta-analysis.Crit Care. 2021 Mar 29;25(1):125. doi: 10.1186/s13054-021-03523-7. Crit Care. 2021. PMID: 33781307 Free PMC article.
-
Accuracy of non-invasive measurement of cardiac output using electrical cardiometry in preterm infants during the transitional period: A comparison with transthoracic Doppler echocardiography.Eur J Pediatr. 2025 Apr 15;184(5):299. doi: 10.1007/s00431-025-06132-6. Eur J Pediatr. 2025. PMID: 40229586 Free PMC article.
-
Cardiac Output Measurement in Neonates and Children Using Noninvasive Electrical Bioimpedance Compared With Standard Methods: A Systematic Review and Meta-Analysis.Crit Care Med. 2022 Jan 1;50(1):126-137. doi: 10.1097/CCM.0000000000005144. Crit Care Med. 2022. PMID: 34325447
-
Noninvasive assessment of cardiac output using thoracic electrical bioimpedance in hemodynamically stable and unstable patients after cardiac surgery: a comparison with pulmonary artery thermodilution.Intensive Care Med. 2006 Dec;32(12):2053-8. doi: 10.1007/s00134-006-0409-x. Epub 2006 Oct 13. Intensive Care Med. 2006. Retraction in: Intensive Care Med. 2011 Jul;37(7):1232. doi: 10.1007/s00134-011-2219-z. PMID: 17039348 Retracted.
Cited by
-
Comparison of noninvasive electrical cardiometry and transpulmonary thermodilution for cardiac output measurement in critically ill patients: a prospective observational study.BMC Anesthesiol. 2025 Mar 13;25(1):123. doi: 10.1186/s12871-025-03005-1. BMC Anesthesiol. 2025. PMID: 40082773 Free PMC article.
-
Non-invasive electrical cardiometry cardiac output monitoring during prehospital helicopter emergency medical care: a feasibility study.J Clin Monit Comput. 2022 Apr;36(2):363-370. doi: 10.1007/s10877-021-00657-5. Epub 2021 Jan 23. J Clin Monit Comput. 2022. PMID: 33486570 Free PMC article.
-
FoCUS and non-invasive hemodynamics monitoring in neonatal sepsis.Eur J Pediatr. 2025 Jun 30;184(7):456. doi: 10.1007/s00431-025-06283-6. Eur J Pediatr. 2025. PMID: 40583086 Free PMC article.
-
Inferior vena cava ultrasound and other techniques for assessment of intravascular and extravascular volume: an update.Clin Kidney J. 2023 Jun 29;16(11):1861-1877. doi: 10.1093/ckj/sfad156. eCollection 2023 Nov. Clin Kidney J. 2023. PMID: 37915939 Free PMC article. Review.
-
Time series analysis of non-invasive hemodynamic monitoring data in neonates with hypoxic-ischemic encephalopathy.Front Pediatr. 2023 Mar 23;11:1112959. doi: 10.3389/fped.2023.1112959. eCollection 2023. Front Pediatr. 2023. PMID: 37033181 Free PMC article.
References
-
- Sun Y, Chai F, Pan C, Romeiser JL, Gan TJ. Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials. Crit Care (London, England) 2017;21(1):141. doi: 10.1186/s13054-017-1728-8. - DOI - PMC - PubMed
-
- Pearse RM, Harrison DA, MacDonald N, Gillies MA, Blunt M, Ackland G, Grocott MP, Ahern A, Griggs K, Scott R, Hinds C, Rowan K. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: a randomized clinical trial and systematic review. JAMA. 2014;311(21):2181–2190. doi: 10.1001/jama.2014.5305. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
