

Clinical and Biological Characterisation of Localised High-risk Prostate Cancer: Results of a Randomised Preoperative Study of a Luteinising Hormone-releasing Hormone Agonist with or Without Abiraterone Acetate plus Prednisone
- PMID: 31176622
- PMCID: PMC7205516
- DOI: 10.1016/j.eururo.2019.05.010
Clinical and Biological Characterisation of Localised High-risk Prostate Cancer: Results of a Randomised Preoperative Study of a Luteinising Hormone-releasing Hormone Agonist with or Without Abiraterone Acetate plus Prednisone
Abstract
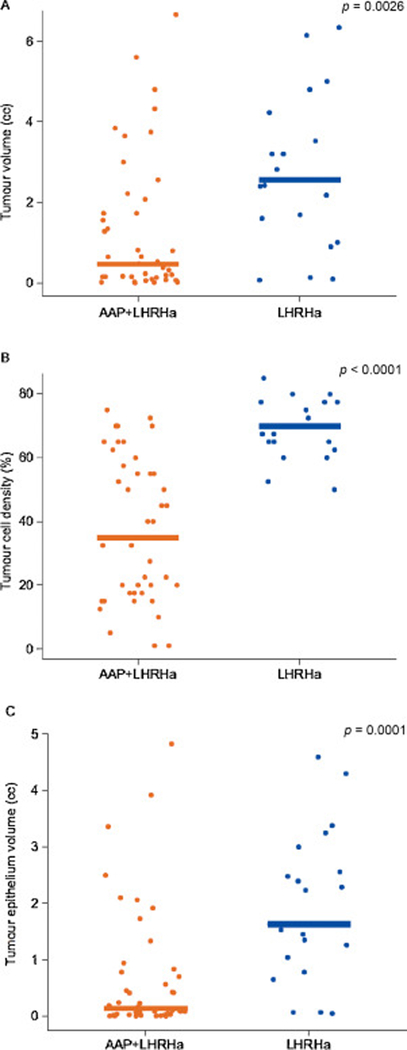
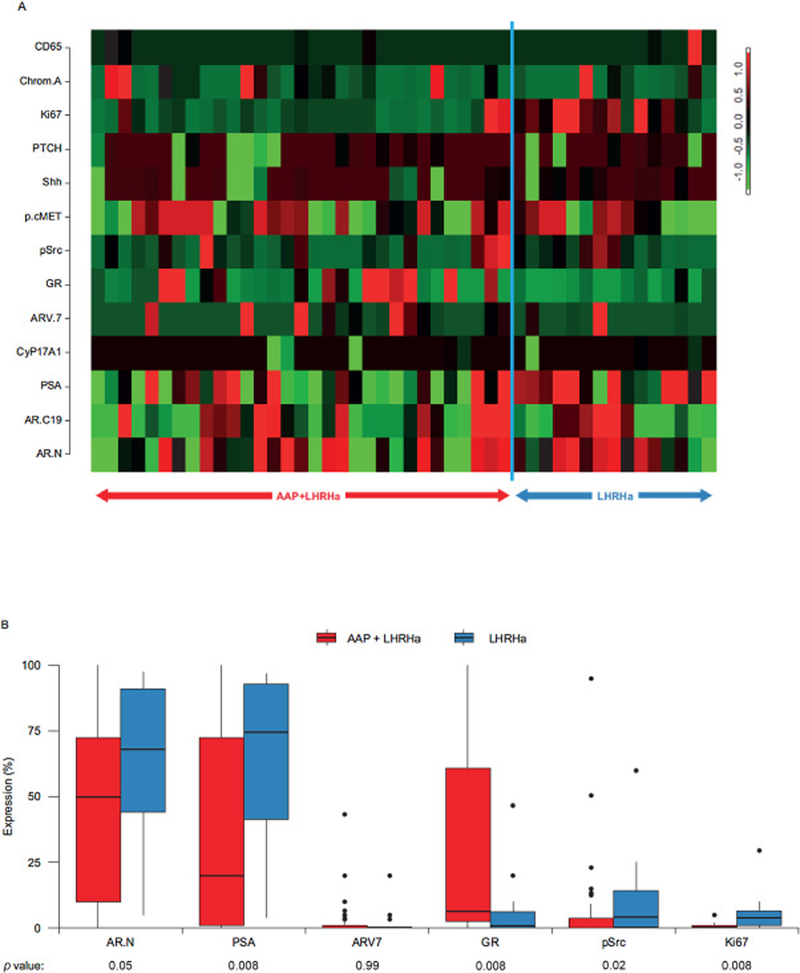
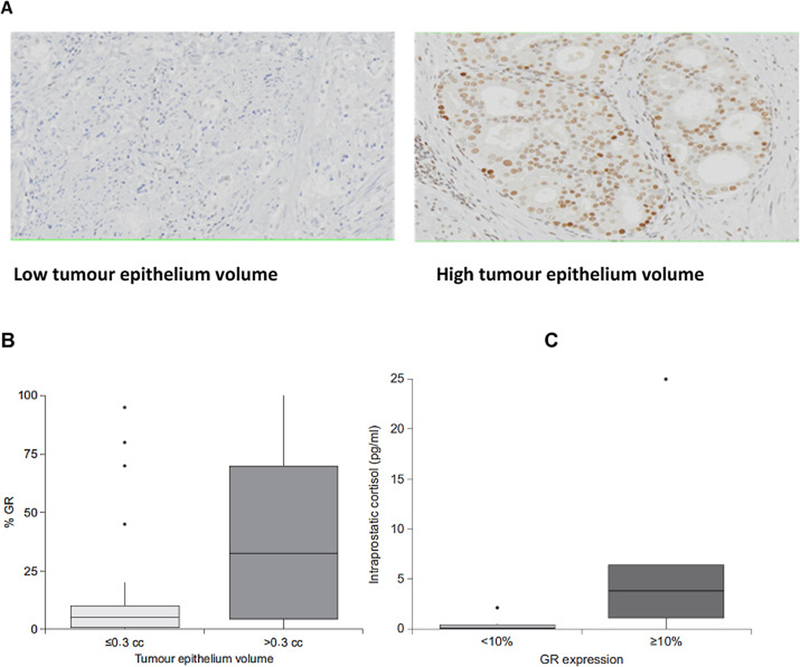
Optimal therapeutic strategy remains an unmet need in localised high-risk prostate cancer (LHRPC). Androgen biosynthesis inhibition in the preoperative setting may improve outcomes. In this single-centre randomised trial, we looked at therapy outcomes of preoperative treatment with abiraterone acetate+prednisone (AAP)+luteinising hormone-releasing hormone agonist (LHRHa) or LHRHa alone followed by radical prostatectomy in 65 men. We did not see a significant difference of organ-confined carcinoma (p=0.27). However, tumour volume measures were significantly lower for AAP+LHRHa treatment (p≤0.001). Of note, lower tumour epithelium volume correlated with improved biochemical recurrence-free survival at ≥4-yr follow-up (p=0.0014). Tumours pretreated with AAP+LHRHa had lower proliferation and androgen signalling expression than LHRHa. On multivariate analysis, glucocorticoid receptor (GR) overexpression correlated with persistent tumours in AAP+LHRHa (p=0.018). The presence of nuclear androgen receptor splice variant (nARV7) correlated with persistent tumours in both arms. No new safety signals were observed. This is the first study investigating the role of preoperative AAP+LHRHa versus LHRHa alone in LHRPC. We report significant cytoreduction by tumour volume measures inversely correlating with biochemical relapse. Validation of these proposed tumour volume measures is planned. A potential role of GR in resistance to androgen biosynthesis inhibition warrants further study. PATIENT SUMMARY: This is the first study of abiraterone acetate plus leuprolide versus leuprolide alone in high-risk localised prostate cancer followed by prostatectomy. Patients in the combination arm had a significantly smaller tumour size.
Keywords: Abiraterone acetate; Androgen deprivation therapy; Androgen receptor; Androgen receptor splice variant; Glucocorticoid receptor; High-risk localised prostate cancer; Neoadjuvant; Preoperative; Radical prostatectomy; Tumour volume.
Copyright © 2019. Published by Elsevier B.V.
Figures
References
-
- Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 2017;377:352–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
