

Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: The Cardiac Rehabilitation Outcome Study in Heart Failure (CROS-HF): A systematic review and meta-analysis
- PMID: 31177833
- PMCID: PMC7272131
- DOI: 10.1177/2047487319854140
Exercise-based cardiac rehabilitation in patients with reduced left ventricular ejection fraction: The Cardiac Rehabilitation Outcome Study in Heart Failure (CROS-HF): A systematic review and meta-analysis
Abstract
Background: In heart failure with reduced left ventricular ejection fraction (HFrEF) patients the effects of exercise-based cardiac rehabilitation on top of state-of-the-art pharmacological and device therapy on mortality, hospitalization, exercise capacity and quality-of-life are not well established.
Design: The design of this study involved a structured review and meta-analysis.
Methods: Evaluation of randomised controlled trials of exercise-based cardiac rehabilitation in HFrEF-patients with left ventricular ejection fraction ≤40% of any aetiology with a follow-up of ≥6 months published in 1999 or later.
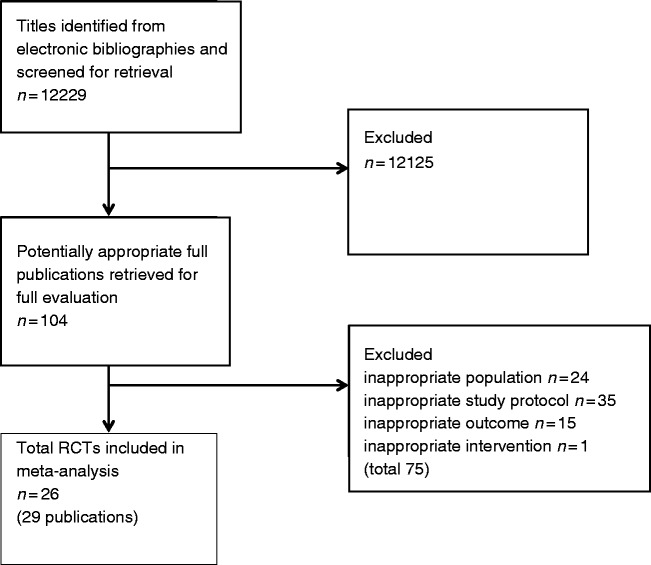
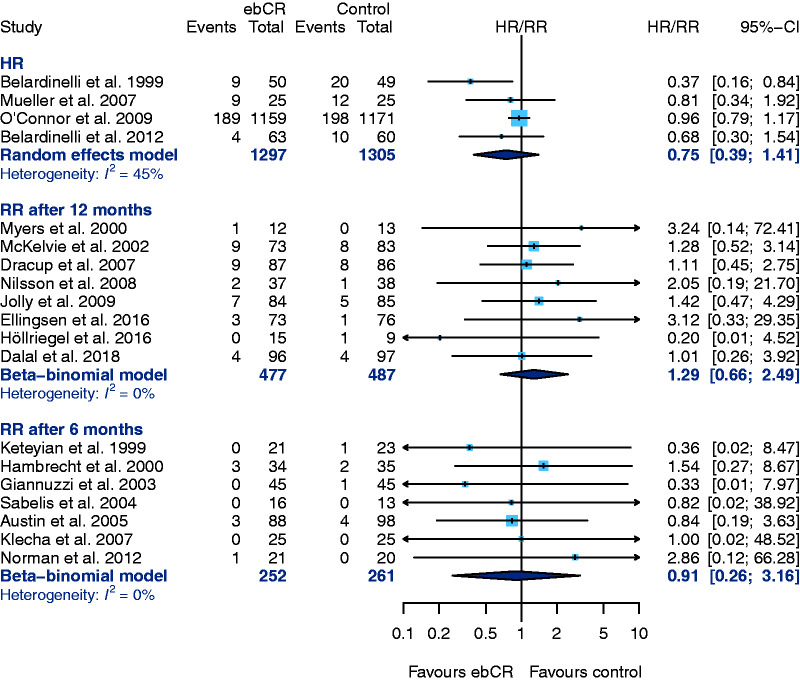
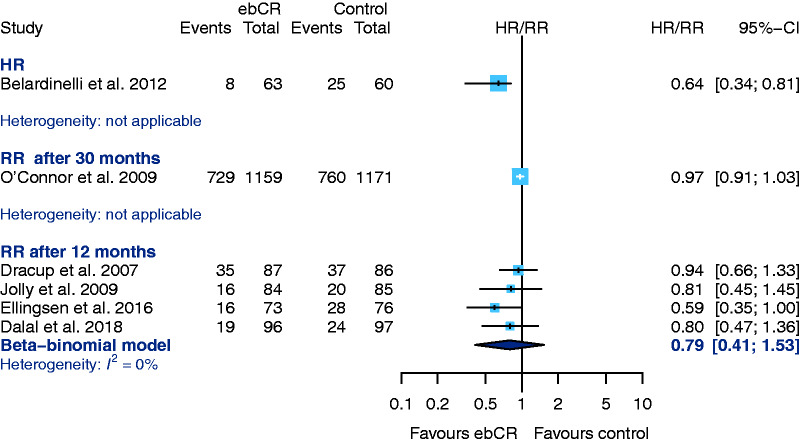
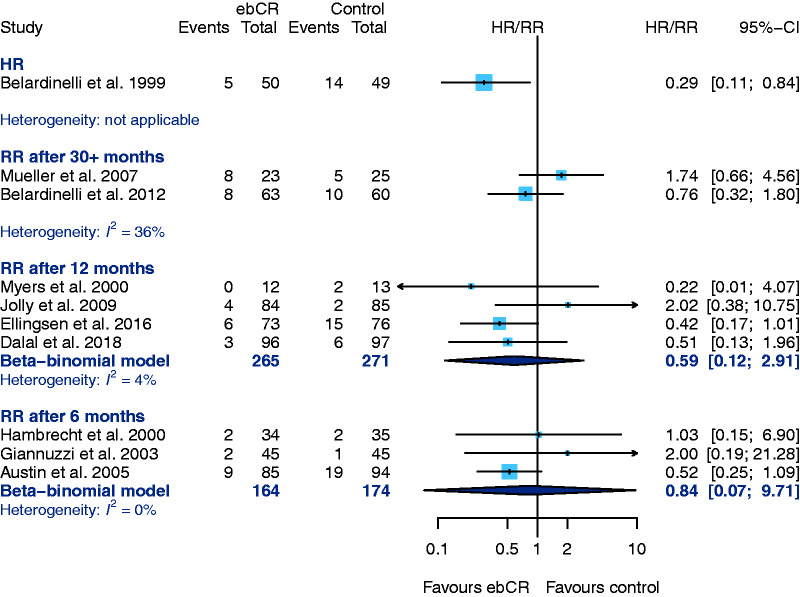
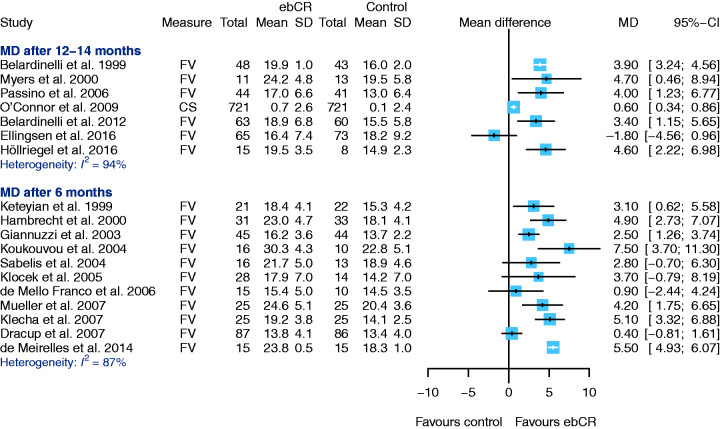
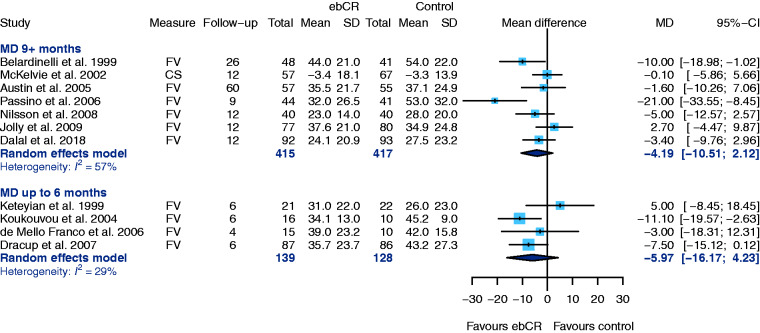
Results: Out of 12,229 abstracts, 25 randomised controlled trials including 4481 HFrEF-patients were included in the final evaluation. Heterogeneity in study population, study design and exercise-based cardiac rehabilitation-intervention was evident. No significant difference in the effect of exercise-based cardiac rehabilitation on mortality compared to control-group was found (hazard ratio 0.75, 95% confidence interval 0.39-1.41, four studies; 12-months follow-up: relative risk 1.29, 95% confidence interval 0.66-2.49, eight studies; six-months follow-up: relative risk 0.91, 95% confidence interval 0.26-3.16, seven studies). In addition there was no significant difference between the groups with respect to 'hospitalization-for-any-reason' (12-months follow-up: relative risk 0.79, 95% confidence interval 0.41-1.53, four studies), or 'hospitalization-due-to-heart-failure' (12-months follow-up: relative risk 0.59, 95% confidence interval 0.12-2.91, four studies; six-months follow-up: relative risk 0.84, 95% confidence interval 0.07-9.71, three studies). All studies show improvement of exercise capacity. Participation in exercise-based cardiac rehabilitation significantly improved quality-of-life as evaluated with the Kansas City Cardiomyopathy Questionnaire: (six-months follow-up: mean difference 1.94, 95% confidence interval 0.35-3.56, two studies), but no significant results emerged for quality-of-life measured by the Minnesota Living with Heart Failure Questionnaire (nine-months or more follow-up: mean difference -4.19, 95% confidence interval -10.51-2.12, seven studies; six-months follow-up: mean difference -5.97, 95% confidence interval -16.17-4.23, four studies).
Conclusion: No association between exercise-based cardiac rehabilitation and mortality or hospitalisation could be observed in HFrEF patients but exercise-based cardiac rehabilitation is likely to improve exercise capacity and quality of life.
Keywords: Meta-analysis; cardiac rehabilitation; exercise training; heart failure; systematic review.
Figures

Comment in
-
Heart failure rehabilitation improves quality of life but we need to offer alternative modes of delivery to increase uptake.Eur J Prev Cardiol. 2020 Dec;27(19):2047-2048. doi: 10.1177/2047487319863507. Epub 2019 Jul 9. Eur J Prev Cardiol. 2020. PMID: 31288538 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18: 891–975. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013; 62: e147–e239. - PubMed
-
- National Institute for Health and Care Excellence: Clinical Guidelines. NG106. Chronic Heart Failure in Adults: Diagnosis and Management. National Guideline Centre (UK). London: National Institute for Health and Care Excellence (UK); September 2018. - PubMed
-
- Somaratne JB, Berry C, McMurray JJ, et al. The prognostic significance of heart failure with preserved left ventricular ejection fraction: A literature-based meta-analysis. Eur J Heart Fail 2009; 11: 855–862. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
