

Thromboelastography or rotational thromboelastometry for bleeding management in adults undergoing cardiac surgery: a systematic review with meta-analysis and trial sequential analysis
- PMID: 31179059
- PMCID: PMC6531758
- DOI: 10.21037/jtd.2019.04.39
Thromboelastography or rotational thromboelastometry for bleeding management in adults undergoing cardiac surgery: a systematic review with meta-analysis and trial sequential analysis
Abstract
Background: Severe bleeding and massive transfusion of blood products may be associated with increased morbidity and mortality of cardiac surgery. A transfusion algorithm incorporating thromboelastography (TEG) or rotational thromboelastometry (ROTEM) can help to determine the appropriate time and target for the use of hemostatic blood products, which may thus reduce the quantity of blood loss as well as blood products transfused.
Methods: We conducted meta-analysis and trial sequential analysis to evaluate the effects of TEG or ROTEM-guided transfusion algorithms vs. standard treatments for patients undergoing cardiac surgery with cardiac pulmonary bypass.
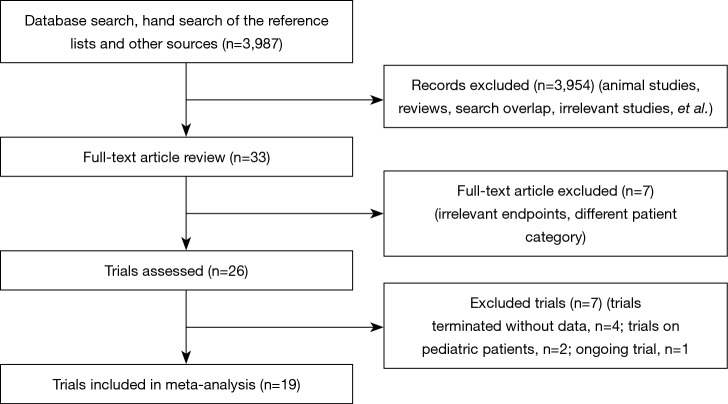
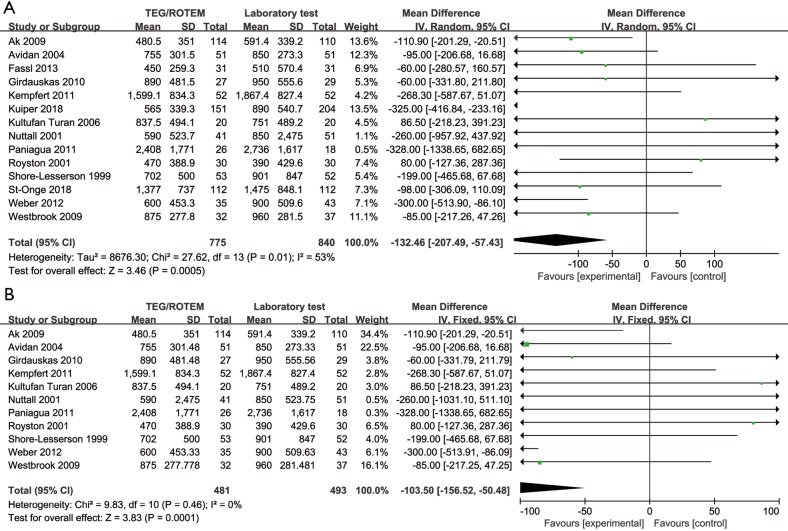
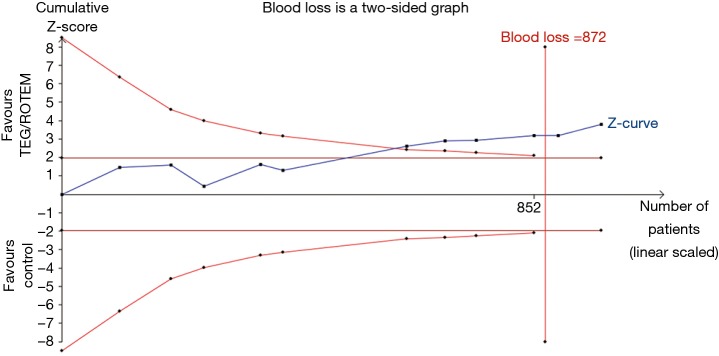
Results: Nineteen studies with a total of 15,320 participants, including 13 randomized controlled trials (RCTs), were included. All-cause mortality was not reduced either in overall studies or in RCTs. Blood loss volume was reduced by 132 mL in overall studies [mean difference (MD): -132.46, 95% CI: -207.49, -57.43; I2 =53%, P<0.01], and by 103 mL in RCTs (MD: -103.50, 95% CI: -156.52, -50.48; I2 =0%, P<0.01). The relative risks (RRs) in RCTs were 0.89 (95% CI: 0.80-0.98; I2 =0%, P=0.02) for red blood cells transfusion, 0.59 (95% CI: 0.42-0.82; I2 =55%, P<0.01) for fresh frozen plasma transfusion, and 0.81 (95% CI: 0.74-0.90; I2 =0%, P<0.01) for platelet transfusion, respectively. Trial sequential analysis of continuous data on blood loss and dichotomous outcomes on transfusion of blood products suggested the benefits of a TEG/ROTEM-guided algorithm.
Conclusions: TEG or ROTEM-guided transfusion strategies may reduce blood loss volume and the transfusion rates in adult patients undergoing cardiac surgery.
Keywords: Thromboelastography (TEG); adult; blood transfusion; cardiac surgical procedures.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Viscoelastic Blood Tests Use in Adult Cardiac Surgery: Meta-Analysis, Meta-Regression, and Trial Sequential Analysis.J Cardiothorac Vasc Anesth. 2020 Jan;34(1):119-127. doi: 10.1053/j.jvca.2019.06.030. Epub 2019 Jun 28. J Cardiothorac Vasc Anesth. 2020. PMID: 31445833
-
Point-of-care thromboelastography/thromboelastometry-based coagulation management in cardiac surgery: a meta-analysis of 8332 patients.J Surg Res. 2016 Jun 15;203(2):424-33. doi: 10.1016/j.jss.2016.03.008. Epub 2016 Mar 26. J Surg Res. 2016. PMID: 27363652
-
Thromboelastography (TEG) or rotational thromboelastometry (ROTEM) to monitor haemostatic treatment in bleeding patients: a systematic review with meta-analysis and trial sequential analysis.Anaesthesia. 2017 Apr;72(4):519-531. doi: 10.1111/anae.13765. Epub 2017 Jan 4. Anaesthesia. 2017. PMID: 28052313
-
Viscoelastic Testing Prior to Non-surgical Procedures Reduces Blood Product Use Without Increasing Bleeding Risk in Cirrhosis.Dig Dis Sci. 2022 Nov;67(11):5290-5299. doi: 10.1007/s10620-021-07376-6. Epub 2022 Feb 5. Dig Dis Sci. 2022. PMID: 35122595 Free PMC article.
-
Shifts of Transfusion Demand in Cardiac Surgery After Implementation of Rotational Thromboelastometry-Guided Transfusion Protocols: Analysis of the HEROES-CS (HEmostasis Registry of patiEntS in Cardiac Surgery) Observational, Prospective Open Cohort Database.J Cardiothorac Vasc Anesth. 2019 Feb;33(2):307-317. doi: 10.1053/j.jvca.2018.08.203. Epub 2018 Aug 29. J Cardiothorac Vasc Anesth. 2019. PMID: 30269889
Cited by
-
The effect of non-point-of-care haemostasis management protocol implementation in cardiac surgery: A systematic review.Transfus Med. 2021 Oct;31(5):328-338. doi: 10.1111/tme.12790. Epub 2021 Jun 6. Transfus Med. 2021. PMID: 34096120 Free PMC article.
-
Effect of rotational thromboelastometry-guided bleeding management in bilateral lung transplantation.JHLT Open. 2024 Jan 17;3:100055. doi: 10.1016/j.jhlto.2024.100055. eCollection 2024 Feb. JHLT Open. 2024. PMID: 40145117 Free PMC article.
-
The role of point of care thromboelastography (TEG) and thromboelastometry (ROTEM) in management of Primary postpartum haemorrhage: A meta-analysis and systematic review.Saudi J Anaesth. 2023 Jan-Mar;17(1):23-32. doi: 10.4103/sja.sja_529_22. Epub 2023 Jan 2. Saudi J Anaesth. 2023. PMID: 37032697 Free PMC article.
-
Prevalence and impact of fibrinolytic dysregulation in patients with acute coronary syndromes.Thromb J. 2021 May 22;19(1):33. doi: 10.1186/s12959-021-00288-5. Thromb J. 2021. PMID: 34022898 Free PMC article.
-
Are Viscoelastometric Assays of Old Generation Ready for Disposal? Comment on Volod et al. Viscoelastic Hemostatic Assays: A Primer on Legacy and New Generation Devices. J. Clin. Med. 2022, 11, 860.J Clin Med. 2023 Jan 6;12(2):477. doi: 10.3390/jcm12020477. J Clin Med. 2023. PMID: 36675406 Free PMC article.
References
LinkOut - more resources
Full Text Sources