

Outcomes following cardiopulmonary resuscitation in an emergency department of a low- and middle-income country
- PMID: 31179917
- PMCID: PMC6326149
- DOI: 10.1186/s12245-018-0200-0
Outcomes following cardiopulmonary resuscitation in an emergency department of a low- and middle-income country
Abstract
Background: Cardiopulmonary resuscitation (CPR) is a key component of emergency care following cardiac arrest. A better understanding of factors that influence CPR outcomes and their prognostic implications would help guide care. A retrospective analysis of 800 adult patients that sustained an in- or out-of-hospital cardiac arrest and underwent CPR in the emergency department of a tertiary care facility in Karachi, Pakistan, between 2008 and 15 was conducted.
Methods: Patient demographics, clinical history, and CPR characteristics data were collected. Logistic regression model was applied to assess predictors of return of spontaneous circulation and survival to discharge. Analysis was conducted using SPSS v.21.0.
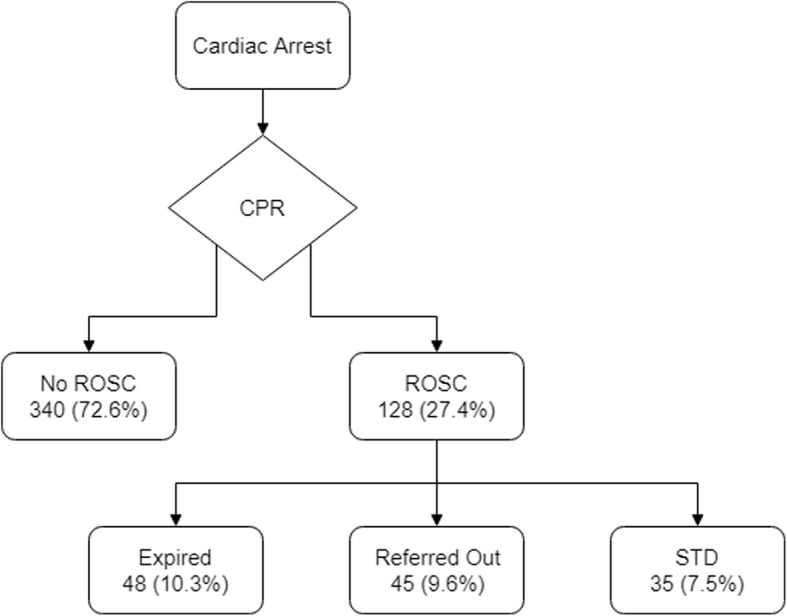
Results: Four hundred sixty-eight patients met the study's inclusion criteria, and overall return of spontaneous circulation and survival to discharge were achieved in 128 (27.4%) and 35 (7.5%) patients respectively. Mean age of patients sustaining return of spontaneous circulation was 52 years and that of survival to discharge was 49 years. The independent predictors of return of spontaneous circulation included age ≤ 49 years, witnessed arrest, ≤ 30 min interval between collapse-to-start, and 1-4 shocks given during CPR (aOR (95% CI) 2.2 (1.3-3.6), 1.9 (1.0-3.7), 14.6 (4.9-43.4), and 3.0 (1.4-6.4) respectively), whereas, age ≤ 52 years, bystander resuscitation, and initial rhythm documented (pulseless electrical activity and ventricular fibrillation) were independent predictors of survival to discharge (aOR (95% CI) 2.5 (0.9-6.5), 1.4 (0.5-3.8), 5.3 (1.5-18.4), and 3.1 (1.0-10.2) respectively).
Conclusion: Our study notes that while the majority of arrests occur out of the hospital, only a small proportion of those arrests receive on-site CPR, which is a key contributor to unfavorable outcomes in this group. It is recommended that effective pre-hospital emergency care systems be established in developing countries which could potentially improve post-arrest outcomes. Younger patients, CPR initiation soon after arrest, presenting rhythm of pulseless ventricular tachycardia and ventricular fibrillation, and those requiring up to four shocks to revive are more likely to achieve favorable outcomes.
Keywords: Cardiopulmonary resuscitation; Return of spontaneous circulation; Survival to discharge.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by Interactive Research and Development’s Institutional Review Board. Anonymity and confidentiality of the participants data was maintained throughout the research. No unauthorized person had access to identifiable patient data.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests associated with this study and/or manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Saklani P, White JA, Klein GJ, Krahn AD. Cardiac arrest and sudden cardiac death. In: Stergiopoulos K, Brown DL, editors. Evidence-based cardiology consult. London: Springer; 2014. pp. 119–132.
-
- Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa) Resuscitation. 2004;63(3):233–249. doi: 10.1016/j.resuscitation.2004.09.008. - DOI - PubMed
-
- Field JM, Kudenchuk PJ, O’Connor R, Vanden Hoek T. The textbook of emergency cardiovascular care and CPR. Philadelphia: Lippincott Williams & Wilkins; 2012.
LinkOut - more resources
Full Text Sources
Miscellaneous
