

Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial
- PMID: 31180155
- PMCID: PMC6851825
- DOI: 10.1111/opo.12621
Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial
Abstract
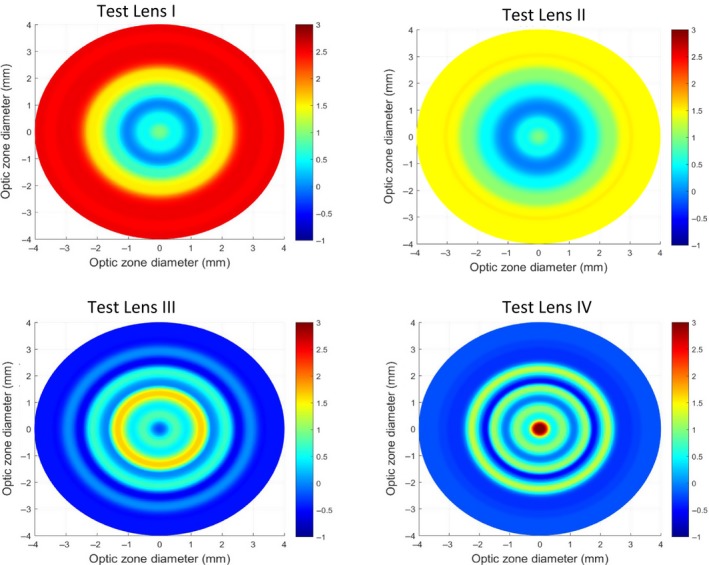
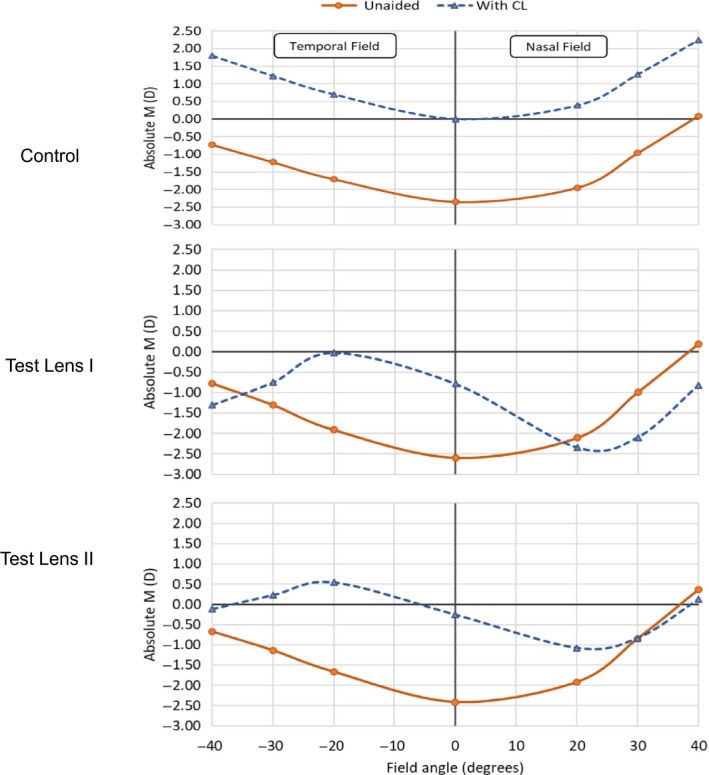
Purpose: We aimed to determine myopia control efficacy with novel contact lenses (CL) that (1) reduced both central and peripheral defocus, and (2) provided extended depth of focus with better global retinal image quality for points on, and anterior to, the retina and degraded for points posterior to the retina.
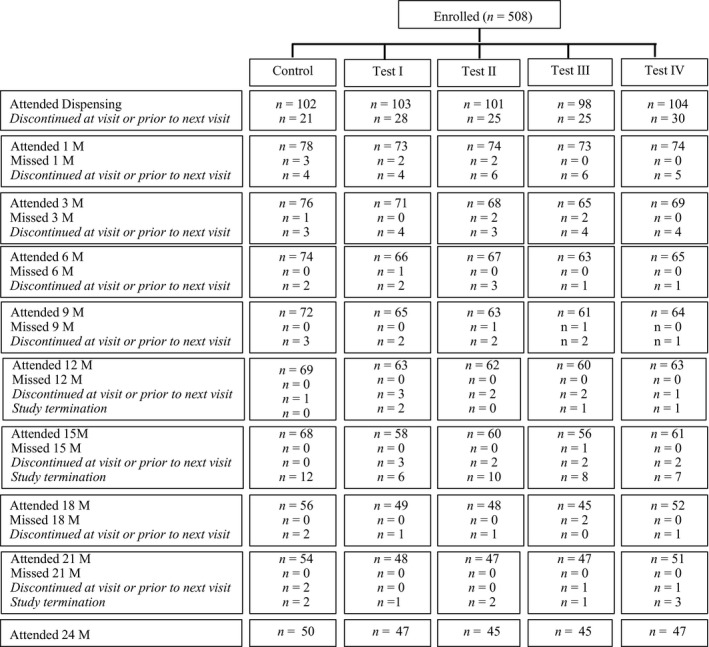
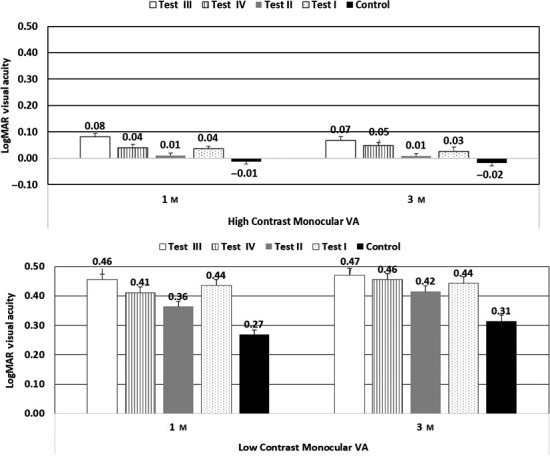
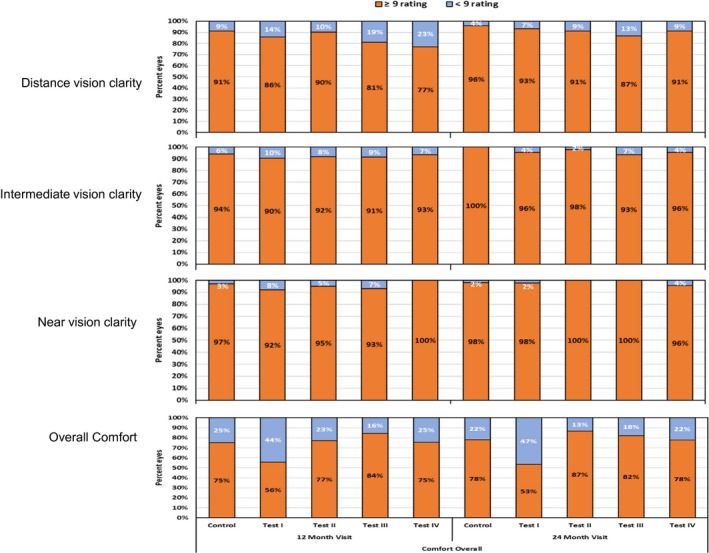
Methods: Children (n = 508, 8-13 years) with cycloplegic spherical equivalent (SE) -0.75 to -3.50D were enrolled in a prospective, double blind trial and randomised to one of five groups: (1) single vision, silicone hydrogel (SH) CL; (2) two groups wearing SH CL that imposed myopic defocus across peripheral and central retina (test CL I and II; +1.00D centrally and +2.50 and +1.50 for CL I and II at 3 mm semi-chord respectively); and (3) two groups wearing extended depth of focus (EDOF) hydrogel CL incorporating higher order aberrations to modulate retinal image quality (test CL III and IV; extended depth of focus of up to +1.75D and +2.50D respectively). Cycloplegic autorefraction and axial length (AL) measurements were conducted at six monthly intervals. Compliance to lens wear was assessed with a diary and collected at each visit. Additionally, subjective responses to various aspects of lens wear were assessed. The trial commenced in February 2014 and was terminated in January 2017 due to site closure. Myopia progression over time between groups was compared using linear mixed models and where needed post hoc analysis with Bonferroni corrections conducted.
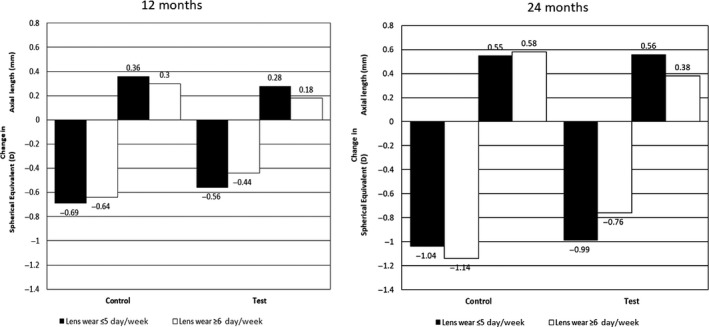
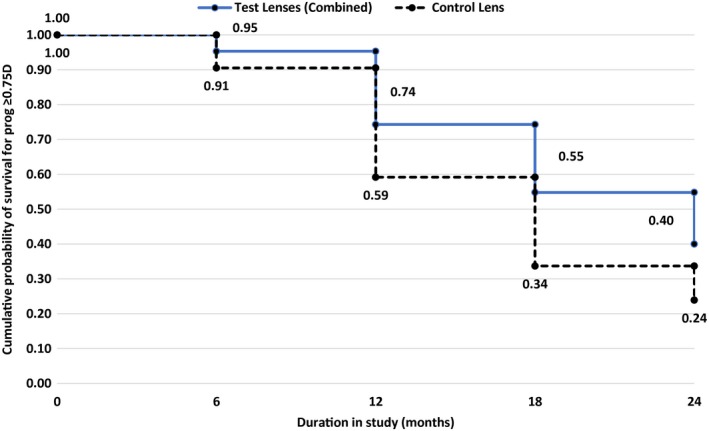
Results: Myopia progressed with control CL -1.12 ± 0.51D/0.58 ± 0.27 mm for SE/AL at 24 months. In comparison, all test CL had reduced progression with SE/AL ranging from -0.78D to -0.87D/0.41-0.46 mm at 24 months (AL: p < 0.05 for all test CL; SE p < 0.05 for test CL III and IV) and represented a reduction in axial length elongation of about 22% to 32% and reduction in spherical equivalent of 24% to 32%. With test CL, a greater slowing ranging from 26% to 43% was observed in compliant wearers (≥6 days per week; Control CL: -0.64D/0.30 mm and -1.14D/0.58 mm vs test CL: -0.42D to -0.47D/0.12-0.18 mm and -0.70 to -0.81D/0.19-0.25 mm at 12 and 24 months respectively).
Conclusions: Contact lenses that either imposed myopic defocus at the retina or modulated retinal image quality resulted in a slower progression of myopia with greater efficacy seen in compliant wearers. Importantly, there was no difference in the myopia control provided by either of these strategies.
Keywords: central and peripheral plus contact lenses; extended depth of focus contact lenses; myopia; progression.
© 2019 The Authors. Ophthalmic and Physiological Optics published by John Wiley & Sons Ltd on behalf of College of Optometrists.
Figures

References
-
- Tideman JW, Snabel MC, Tedja MS et al Association of zxial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol 2016; 134: 1355–1363. - PubMed
-
- Mitchell P, Hourihan F, Sandbach J & Wang JJ. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology 1999; 106: 2010–2015. - PubMed
-
- Xu L, Wang Y, Wang S, Wang Y & Jonas JB. High myopia and glaucoma susceptibility the Beijing Eye Study. Ophthalmology 2007; 114: 216–220. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
