

Cardiopulmonary Testing Before Lung Resection: What Are Thoracic Surgeons Doing?
- PMID: 31181202
- PMCID: PMC11329212
- DOI: 10.1016/j.athoracsur.2019.04.057
Cardiopulmonary Testing Before Lung Resection: What Are Thoracic Surgeons Doing?
Abstract
Background: Cardiopulmonary assessment for lung resection is important for risk stratification, and the American College of Chest Physicians (ACCP) guidelines provide decision support. We ascertained the cardiopulmonary assessment practices of thoracic surgeons and determined whether they are guideline concordant.
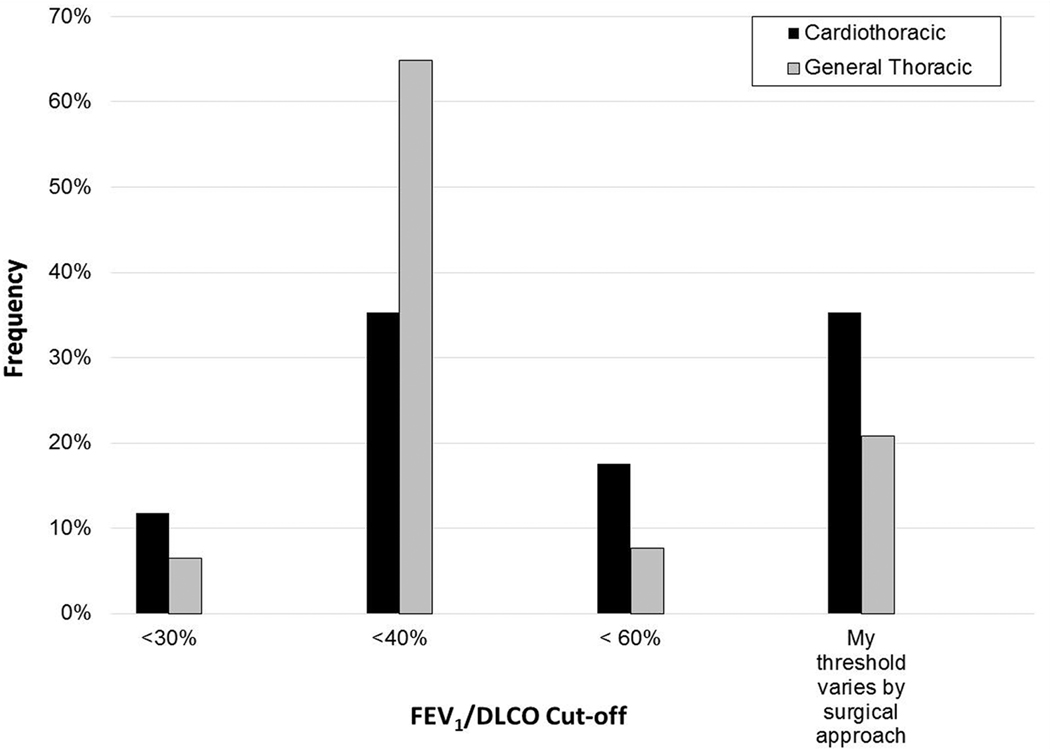
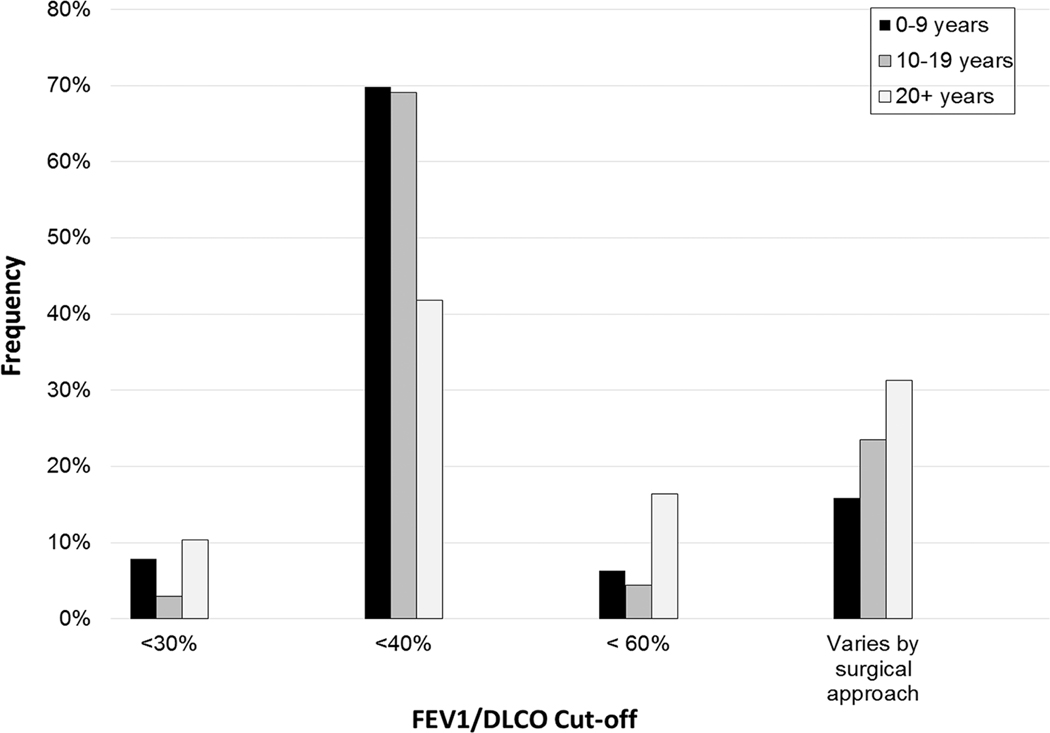
Methods: An anonymous survey was emailed to 846 thoracic surgeons who participate in The Society of Thoracic Surgeons General Thoracic Surgery Database. We analyzed survey responses by practice type (general thoracic [GT] versus cardiothoracic [CT]) and years in practice (0-9, 10-19, and ≥20) with the use of contingency tables. We compared adherence of survey responses with the guidelines.
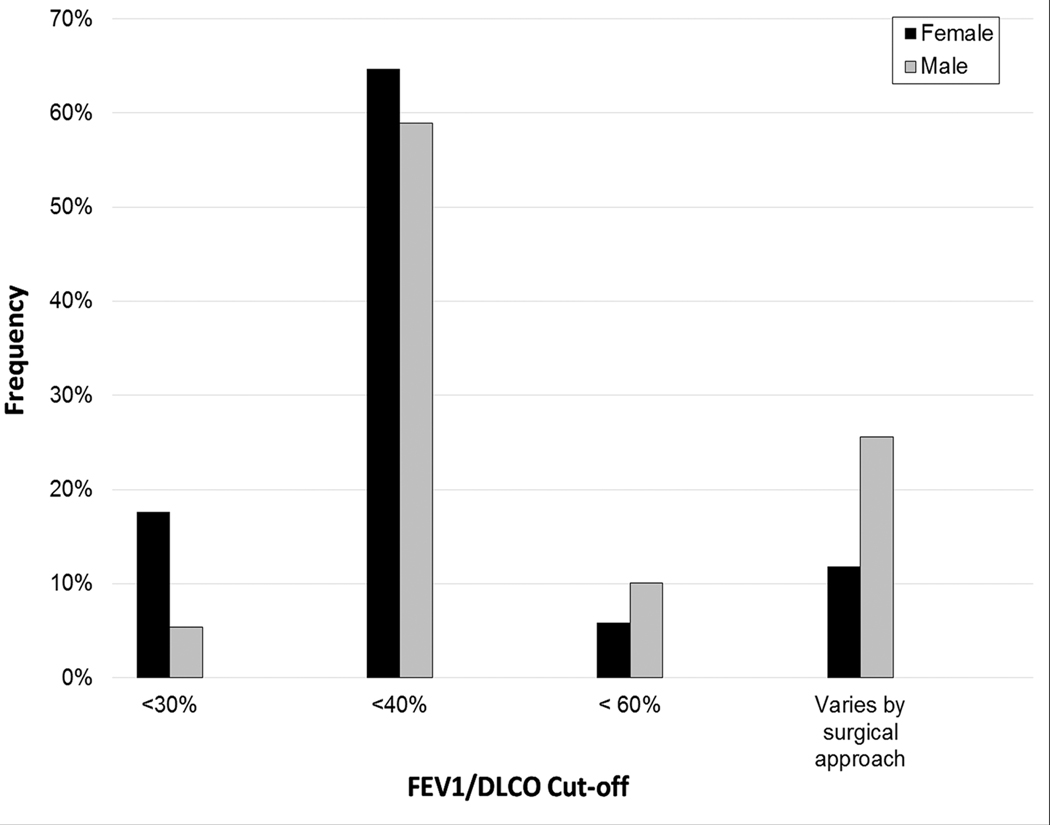
Results: The response rate was 24.0% (n = 203). Most surgeons (n = 121, 59.6%) cited a predicted postoperative forced expiratory volume in 1 second or diffusing capacity of lung for carbon monoxide threshold of 40% for further evaluation. Experienced surgeons (≥20 years) were more likely to have a threshold that varies by surgical approach (31.3% versus 23.5% with 10-19 years of experience and 15.9% for 0-9 years of experience, P = .007). Overall, 52.2% refer patients with cardiovascular risk factors to cardiology and 42.9% refer patients with abnormal stress testing. CT surgeons were more likely to refer all patients to cardiology than GT surgeons (17.6% versus 2.4%, P < .001). Only one respondent (0.5%) was 100% adherent to the ACCP guidelines, and 4.4% and 45.8% were 75% and 50% adherent, respectively.
Conclusions: Among thoracic surgeons, there is variation in preoperative cardiopulmonary assessment practices, with differences by practice type and years in practice, and marked discordance with the ACCP guidelines. Further study of guideline adherence linked to postoperative morbidity and mortality is warranted to determine whether adherence affects outcomes.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Cancer Stat Facts: Lung and Bronchus Cancer. Natl Cancer Inst Surveillance, Epidemiol End Results Progr 2018. https://seer.cancer.gov/statfacts/html/lungb.html (accessed September 21, 2018).
-
- Licker MJ, Widikker I, Robert J, Frey J-G, Spiliopoulos A, Ellenberger C, et al. Operative Mortality and Respiratory Complications After Lung Resection for Cancer: Impact of Chronic Obstructive Pulmonary Disease and Time Trends. Ann Thorac Surg 2006. doi: 10.1016/j.athoracsur.2005.11.048. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
