

Cardiovascular Events and Mortality in White Coat Hypertension: A Systematic Review and Meta-analysis
- PMID: 31181575
- PMCID: PMC6736754
- DOI: 10.7326/M19-0223
Cardiovascular Events and Mortality in White Coat Hypertension: A Systematic Review and Meta-analysis
Abstract
Background: The long-term cardiovascular risk of isolated elevated office blood pressure (BP) is unclear.
Purpose: To summarize the risk for cardiovascular events and all-cause mortality associated with untreated white coat hypertension (WCH) and treated white coat effect (WCE).
Data sources: PubMed and EMBASE, without language restriction, from inception to December 2018.
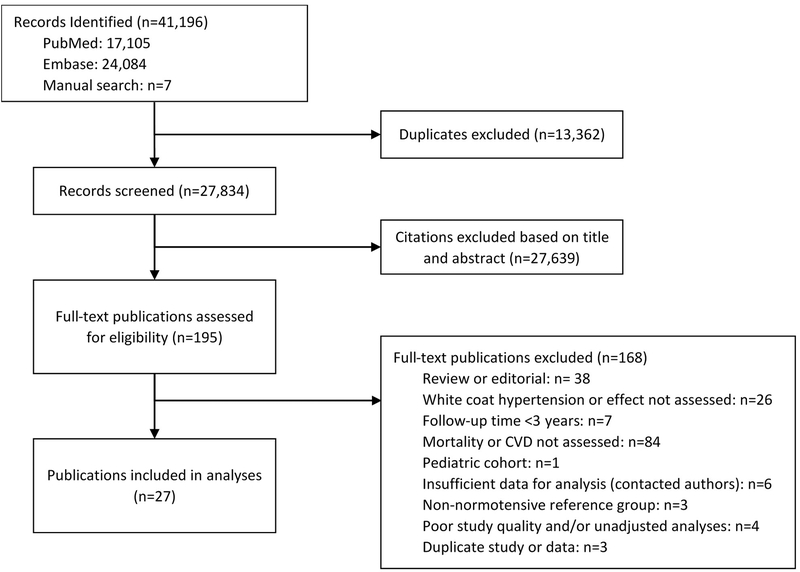
Study selection: Observational studies with at least 3 years of follow-up evaluating the cardiovascular risk of WCH or WCE compared with normotension.
Data extraction: 2 investigators independently extracted study data and assessed study quality.
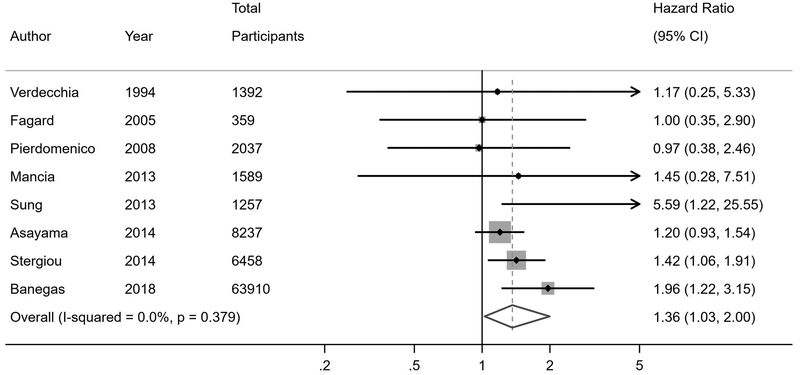
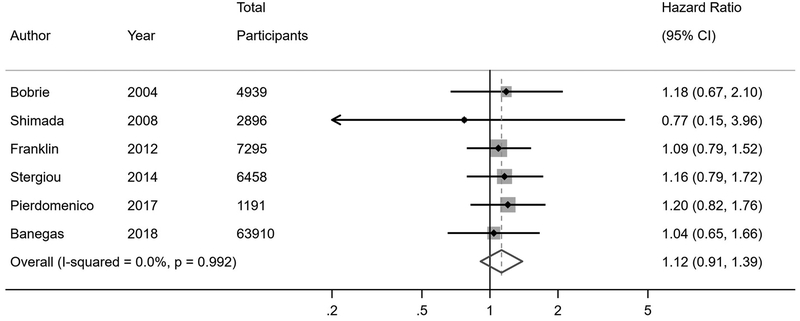
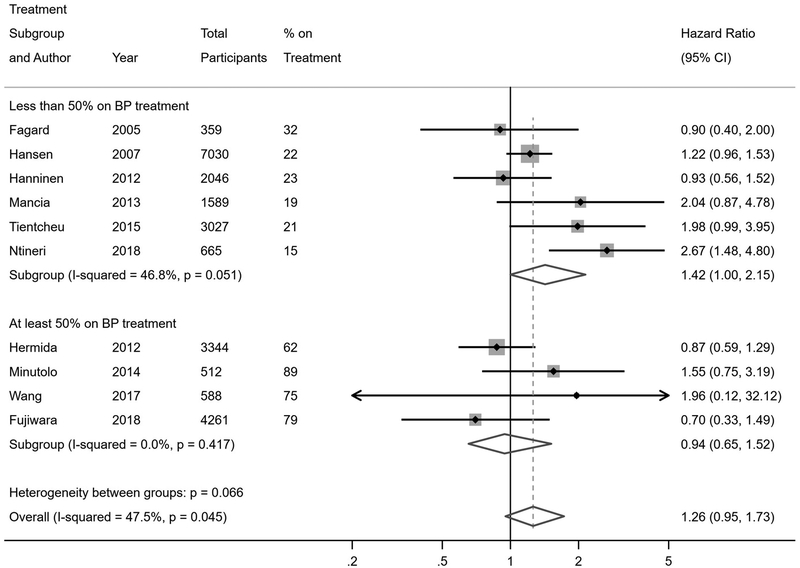
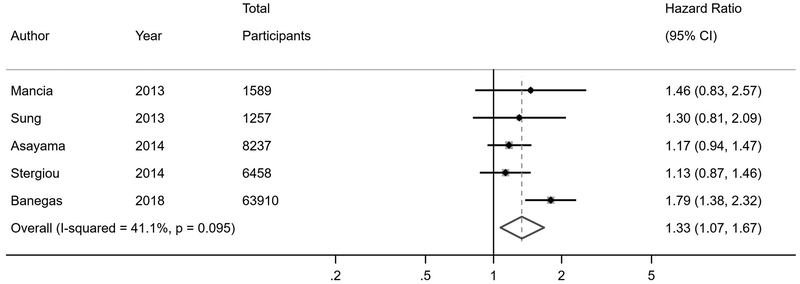
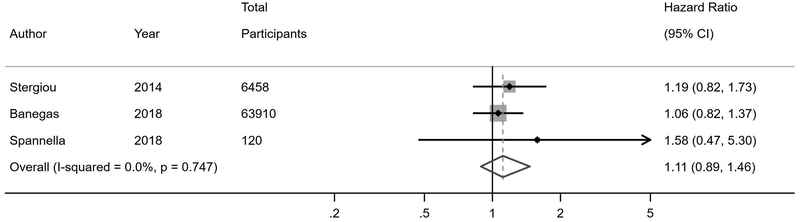
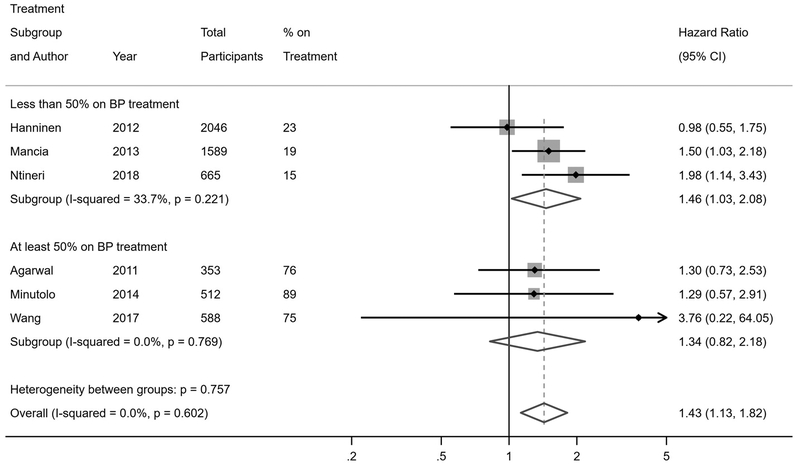
Data synthesis: 27 studies were included, comprising 25 786 participants with untreated WCH or treated WCE and 38 487 with normal BP followed for a mean of 3 to 19 years. Compared with normotension, untreated WCH was associated with an increased risk for cardiovascular events (hazard ratio [HR], 1.36 [95% CI, 1.03 to 2.00]), all-cause mortality (HR, 1.33 [CI, 1.07 to 1.67]), and cardiovascular mortality (HR, 2.09 [CI, 1.23 to 4.48]); the risk for WCH was attenuated in studies that included stroke in the definition of cardiovascular events (HR, 1.26 [CI, 1.00 to 1.54]). No significant association was found between treated WCE and cardiovascular events (HR, 1.12 [CI, 0.91 to 1.39]), all-cause mortality (HR, 1.11 [CI, 0.89 to 1.46]), or cardiovascular mortality (HR, 1.04 [CI, 0.65 to 1.66]). The findings persisted across several sensitivity analyses.
Limitation: Paucity of studies evaluating isolated cardiac outcomes or reporting participant race/ethnicity.
Conclusion: Untreated WCH, but not treated WCE, is associated with an increased risk for cardiovascular events and all-cause mortality. Out-of-office BP monitoring is critical in the diagnosis and management of hypertension.
Primary funding source: National Institutes of Health.
Figures
Comment in
-
Should Out-of-Office Monitoring Be Performed for Detecting White Coat Hypertension?Ann Intern Med. 2019 Jun 18;170(12):890-892. doi: 10.7326/M19-1134. Epub 2019 Jun 11. Ann Intern Med. 2019. PMID: 31181573 No abstract available.
-
Cardiovascular Events and Mortality in White Coat Hypertension.Ann Intern Med. 2019 Oct 15;171(8):602-603. doi: 10.7326/L19-0523. Ann Intern Med. 2019. PMID: 31610568 No abstract available.
-
Cardiovascular Events and Mortality in White Coat Hypertension.Ann Intern Med. 2019 Oct 15;171(8):603-604. doi: 10.7326/L19-0524. Ann Intern Med. 2019. PMID: 31610569 Free PMC article. No abstract available.
References
-
- Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392(10159):1923–94. - PMC - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):e13–e115. - PubMed
-
- Siu AL, Force USPST. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163(10):778–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources