

Time-Dependent Myocardial Necrosis in Patients With ST-Segment-Elevation Myocardial Infarction Without Angiographic Collateral Flow Visualized by Cardiac Magnetic Resonance Imaging: Results From the Multicenter STEMI-SCAR Project
- PMID: 31181983
- PMCID: PMC6645633
- DOI: 10.1161/JAHA.119.012429
Time-Dependent Myocardial Necrosis in Patients With ST-Segment-Elevation Myocardial Infarction Without Angiographic Collateral Flow Visualized by Cardiac Magnetic Resonance Imaging: Results From the Multicenter STEMI-SCAR Project
Abstract
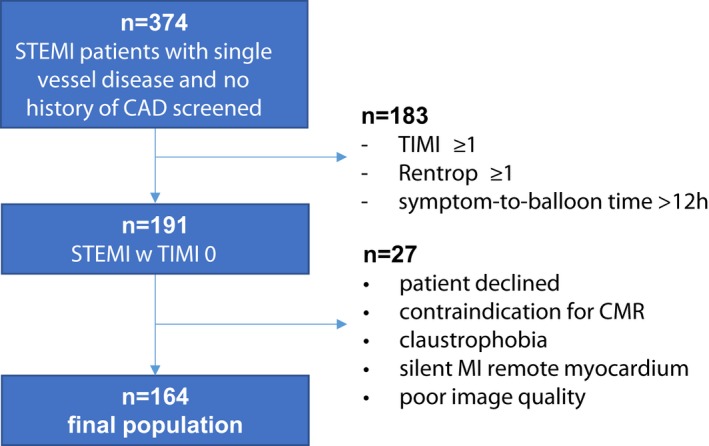
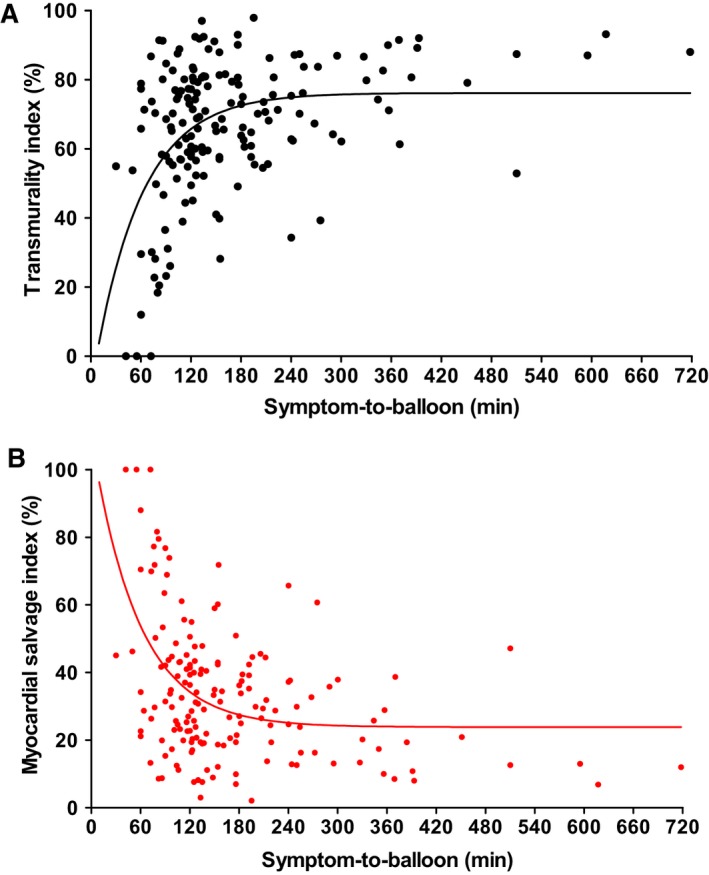
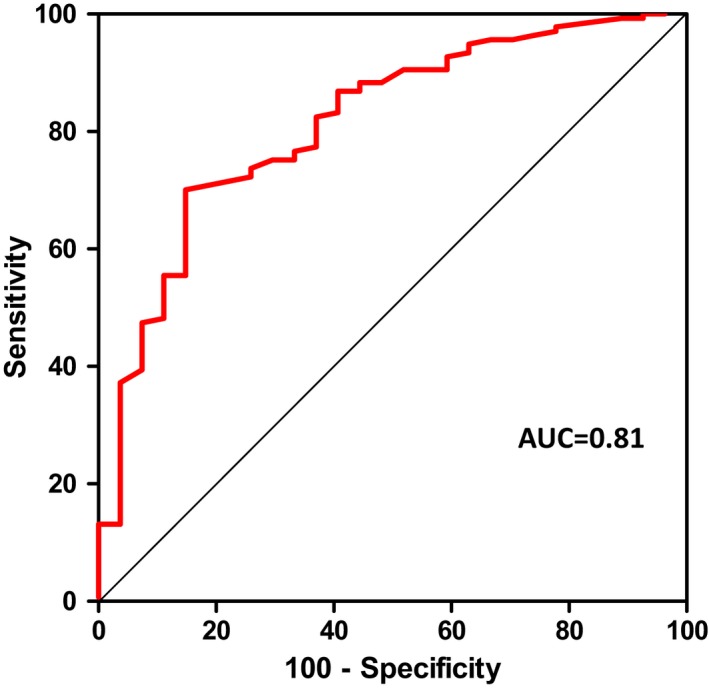
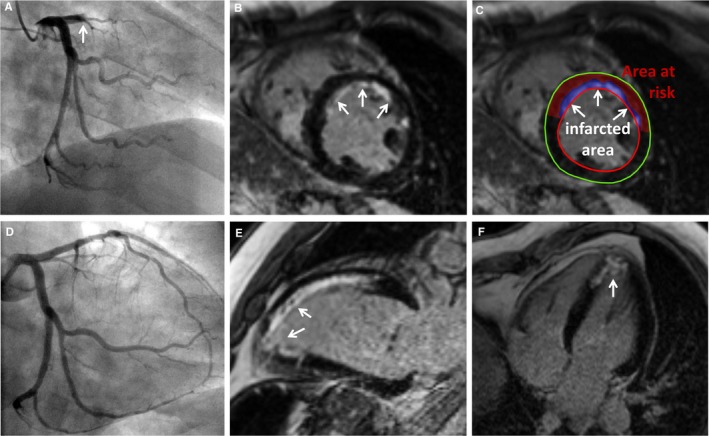
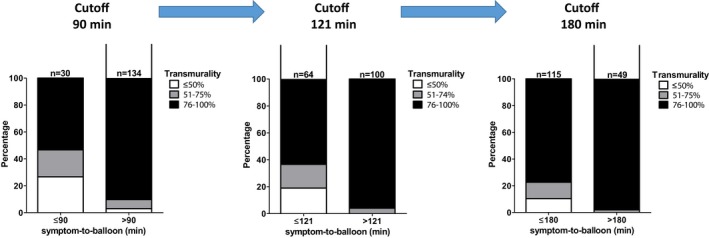
Background Acute complete occlusion of a coronary artery results in progressive ischemia, moving from the endocardium to the epicardium (ie, wavefront). Dependent on time to reperfusion and collateral flow, myocardial infarction ( MI ) will manifest, with transmural MI portending poor prognosis. Late gadolinium enhancement cardiac magnetic resonance imaging can detect MI with high diagnostic accuracy. Primary percutaneous coronary intervention is the preferred reperfusion strategy in patients with ST -segment-elevation MI with <12 hours of symptom onset. We sought to visualize time-dependent necrosis in a population with ST -segment-elevation MI by using late gadolinium enhancement cardiac magnetic resonance imaging (STEMI-SCAR project). Methods and Results ST -segment-elevation MI patients with single-vessel disease, complete occlusion with TIMI (Thrombolysis in Myocardial Infarction) score 0, absence of collateral flow (Rentrop score 0), and symptom onset <12 hours were consecutively enrolled. Using late gadolinium enhancement cardiac magnetic resonance imaging, the area at risk and infarct size, myocardial salvage index, transmurality index, and transmurality grade (0-50%, 51-75%, 76-100%) were determined. In total, 164 patients (aged 54±11 years, 80% male) were included. A receiver operating characteristic curve (area under the curve: 0.81) indicating transmural necrosis revealed the best diagnostic cutoff for a symptom-to-balloon time of 121 minutes: patients with >121 minutes demonstrated increased infarct size, transmurality index, and transmurality grade (all P<0.01) and decreased myocardial salvage index ( P<0.001) versus patients with symptom-to-balloon times ≤121 minutes. Conclusions In MI with no residual antegrade and no collateral flow, immediate reperfusion is vital. A symptom-to-balloon time of >121 minutes causes a high grade of transmural necrosis. In this pure ST -segment-elevation MI population, time to reperfusion to salvage myocardium was less than suggested by current guidelines.
Keywords: ST‐segment–elevation myocardial infarction; cardiac magnetic resonance imaging; coronary artery disease; necrosis.
Figures
Comment in
-
Targeting an Ischemic Time <120 Minutes in ST-Segment-Elevation Myocardial Infarction.J Am Heart Assoc. 2019 Jun 18;8(12):e013067. doi: 10.1161/JAHA.119.013067. Epub 2019 Jun 11. J Am Heart Assoc. 2019. PMID: 31181986 Free PMC article. No abstract available.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimský P; ESC Scientific Document Group . 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. - PubMed
-
- Reimer KA, Jennings RB. The “wavefront phenomenon” of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979;40:633–644. - PubMed
-
- Seiler C, Kirkeeide RL, Gould KL. Measurement from arteriograms of regional myocardial bed size distal to any point in the coronary vascular tree for assessing anatomic area at risk. J Am Coll Cardiol. 1993;21:783–797. - PubMed
-
- Gersh BJ, Stone GW, White HD, Holmes DR Jr. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future? JAMA. 2005;293:979–986. - PubMed
-
- Eitel I, Desch S, de Waha S, Fuernau G, Gutberlet M, Schuler G, Thiele H. Long‐term prognostic value of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. Heart. 2011;97:2038–2045. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
