

Ovarian transposition before radiotherapy in cervical cancer patients: functional outcome and the adequate dose constraint
- PMID: 31182114
- PMCID: PMC6558909
- DOI: 10.1186/s13014-019-1312-2
Ovarian transposition before radiotherapy in cervical cancer patients: functional outcome and the adequate dose constraint
Abstract
Background: The data regarding a transposed ovary in intensity-modulated radiotherapy (IMRT) are not sufficient. Here we aim to investigate the adequate dose constraint of ovarian transposition before radiotherapy in cervical cancer patients.
Methods: This was a retrospective analysis of 118 patients with cervical cancer who received a radical hysterectomy and ovarian transposition before pelvic irradiation from April 2012 to July 2017. A total of 105 patients underwent IMRT with a limited radiation dose to the ovaries; 48 of these patients received unilateral ovary limitation, while 57 received bilateral ovary limitations. Patient follow up regarding sex hormone levels (estrogen [E2], follicle stimulating hormone [FSH]) and menopausal symptoms was completed one year after their radiation therapy.
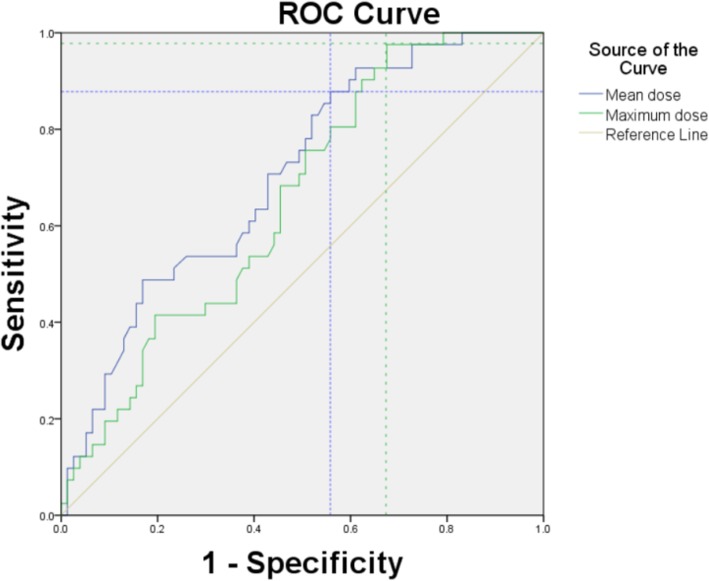
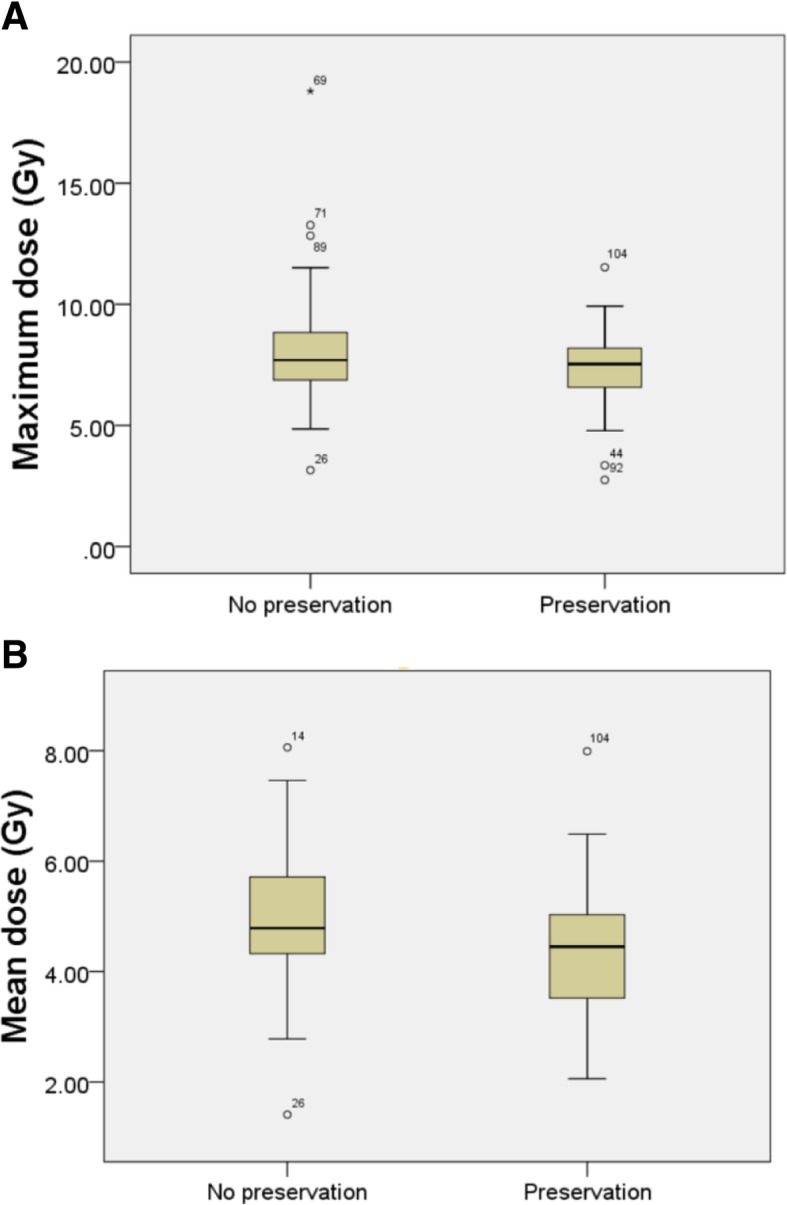
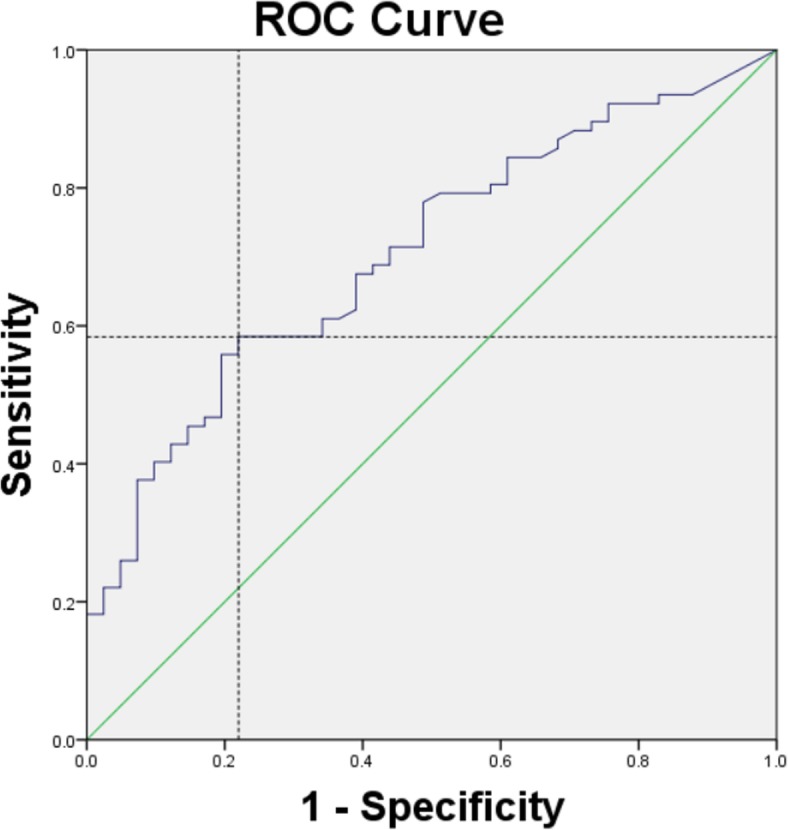
Results: A total of 41 out of 105 patients (39.0%) who underwent IMRT with a limited radiation dose to the ovaries preserved their normal ovarian function. The cutoff dose of comparatively lower side ovarian maximum dose was 9.985Gy and the cutoff of mean dose was 5.32Gy. The optimal dose-volume constrains to ovaries was V5.5 < 29.65%. Age ≤ 38 (P = 0.001) was an independent predictors of ovarian function, while limited ovarian side numbers were excluded.
Conclusion: Using IMRT, preservation of ovarian function was possible when the limited dose was as low as possible to the ovaries regardless of bilateral or unilateral limitation to the ovaries. The ovarian maximum dose of less than 9.985Gy, the mean dose less than 5.32Gy and V5.5 < 29.65% could be better at preventing ovarian dysfunction. Patients younger than 38 years old were more likely to keep normal ovarian function while limited ovarian side numbers did not appear to exert an obvious effect.
Keywords: Cervical cancer; Ovarian function; Ovarian transposition; Radiotherapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The relationship between ovarian function and ovarian limited dose in radiotherapy postoperation of ovarian transposition in young patients with cervical cancer.Cancer Med. 2017 Mar;6(3):508-515. doi: 10.1002/cam4.924. Epub 2017 Feb 17. Cancer Med. 2017. PMID: 28211638 Free PMC article.
-
Association between the location of transposed ovary and ovarian dose in patients with cervical cancer treated with postoperative pelvic radiotherapy.Radiat Oncol. 2019 Dec 16;14(1):230. doi: 10.1186/s13014-019-1437-3. Radiat Oncol. 2019. PMID: 31842971 Free PMC article.
-
Strategies for reducing ovarian dose in volumetric modulated arc therapy (VMAT) for postoperative uterine cervical cancer.Br J Radiol. 2018 Jan;91(1081):20160777. doi: 10.1259/bjr.20160777. Epub 2017 Nov 3. Br J Radiol. 2018. PMID: 29072492 Free PMC article.
-
Ovarian transposition in patients with cervical cancer prior to pelvic radiotherapy: a systematic review.Int J Gynecol Cancer. 2021 Mar;31(3):360-370. doi: 10.1136/ijgc-2020-001774. Int J Gynecol Cancer. 2021. PMID: 33649003
-
The role of oophoropexy in patients with gynecological cancer who need radiation therapy.Int J Gynecol Cancer. 2022 Mar;32(3):380-388. doi: 10.1136/ijgc-2021-002471. Int J Gynecol Cancer. 2022. PMID: 35256427 Review.
Cited by
-
Significance of ovarian transposition in the preservation of ovarian function for young cervical cancer patients undergoing postoperative volumetric modulated radiotherapy.Ann Transl Med. 2021 Dec;9(23):1717. doi: 10.21037/atm-21-2909. Ann Transl Med. 2021. PMID: 35071411 Free PMC article.
-
Successful Pre-Treatment Ovarian Fresh Tissue Transplantation in a Cervical Cancer Patient Undergoing Radiation Therapy: A Case Report.Cureus. 2023 Aug 14;15(8):e43472. doi: 10.7759/cureus.43472. eCollection 2023 Aug. Cureus. 2023. PMID: 37711948 Free PMC article.
-
Factors Associated With Premature Ovarian Insufficiency in Young Women With Locally Advanced Rectal Cancer Treated With Pelvic Radiation Therapy.Adv Radiat Oncol. 2021 Sep 20;7(1):100801. doi: 10.1016/j.adro.2021.100801. eCollection 2022 Jan-Feb. Adv Radiat Oncol. 2021. PMID: 35071829 Free PMC article.
-
Estimated radiation doses to ovarian and uterine organs in breast cancer irradiation using radio-photoluminescent glass dosimeters (RPLDs).J Med Radiat Sci. 2021 Jun;68(2):167-174. doi: 10.1002/jmrs.445. Epub 2020 Oct 20. J Med Radiat Sci. 2021. PMID: 33078910 Free PMC article.
-
Oncological Ligand-Target Binding Systems and Developmental Approaches for Cancer Theranostics.Mol Biotechnol. 2021 Mar;63(3):167-183. doi: 10.1007/s12033-020-00296-2. Epub 2021 Jan 9. Mol Biotechnol. 2021. PMID: 33423212 Review.
References
-
- Motoki Y, Mizushima S, Taguri M, Takahashi K, Asano R, Kato H, et al. Increasing trends in cervical cancer mortality among young Japanese women below the age of 50 years: an analysis using the Kanagawa population-based Cancer registry, 1975-2012. Cancer Epidemiol. 2015;39(5):700–706. doi: 10.1016/j.canep.2015.08.001. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
