

Patterns of Psychiatric Comorbidity and Genetic Correlations Provide New Insights Into Differences Between Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder
- PMID: 31182215
- PMCID: PMC6764861
- DOI: 10.1016/j.biopsych.2019.04.021
Patterns of Psychiatric Comorbidity and Genetic Correlations Provide New Insights Into Differences Between Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder
Erratum in
-
Erratum.Biol Psychiatry. 2019 Oct 15;86(8):647. doi: 10.1016/j.biopsych.2019.07.025. Biol Psychiatry. 2019. PMID: 31558221 Free PMC article. No abstract available.
Abstract
Background: Attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) share common genetic factors but seem to have specific patterns of psychiatric comorbidities. There are few systematic studies on adults; therefore, we compared psychiatric comorbidities in adults with these two neurodevelopmental disorders using population-based data and analyzed their genetic correlations to evaluate underlying factors.
Methods: Using data from Norwegian registries, we assessed patterns of psychiatric disorders in adults with ADHD (n = 38,636; 2.3%), ASD (n = 7528; 0.4%), and both diagnoses (n = 1467; 0.1%) compared with the remaining adult population (n = 1,653,575). We calculated their prevalence ratios (PRs) and differences using Poisson regression, also examining sex-specific relations. Genetic correlations (rg) among ADHD, ASD, and the examined psychiatric disorders were calculated by linkage disequilibrium score regression, exploiting summary statistics from relevant genome-wide association studies.
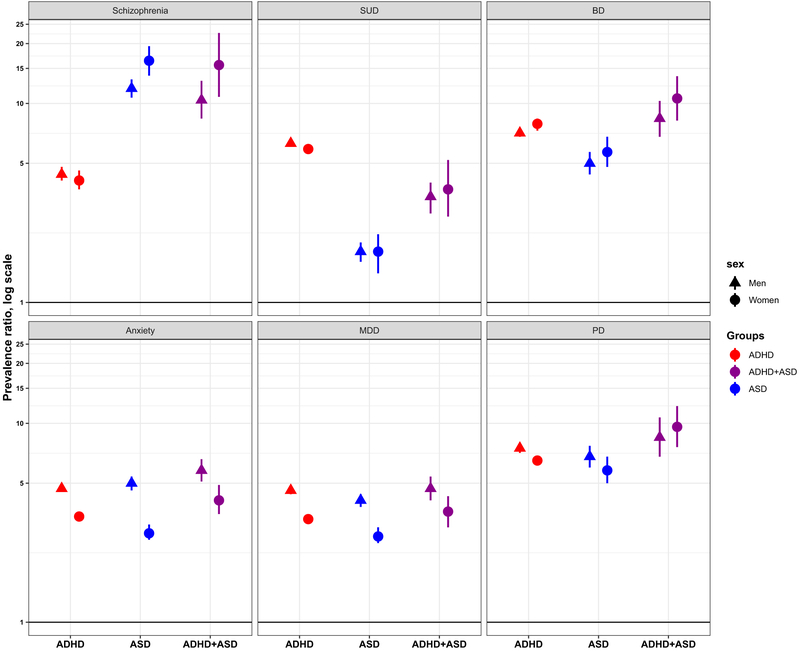
Results: For all psychiatric comorbidities, PRs differed between ADHD and ASD. Associations were strongest in individuals with ADHD and ADHD+ASD for most comorbidities, in both men and women. The relative prevalence increase of substance use disorder was three times larger in ADHD than in ASD (PRADHD, 6.2; 95% confidence interval [CI], 6.1-6.4; PRASD, 1.9; 95% CI, 1.7-2.2; p < .001); however, the opposite was true for schizophrenia (PRASD, 13.9; 95% CI, 12.7-15.2; PRADHD, 4.4; 95% CI, 4.1-4.7; p < .001). Genetic correlations supported these patterns but were significantly different between ADHD and ASD only for the substance use disorder proxies and personality traits (p < .006 for all).
Conclusions: Adults with ADHD, ASD, or both ADHD and ASD have specific patterns of psychiatric comorbidities. This may partly be explained by differences in underlying genetic factors.
Keywords: ADHD; ASD; Genetics; Psychiatric comorbidity; SUD; Schizophrenia.
Copyright © 2019 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
JH has served as a speaker for Eli Lilly, HB Pharma, and Shire. The other authors report no biomedical financial interests or potential conflicts of interest.
Figures


Comment in
-
Large-Scale Population-Based Assessment of Psychiatric Comorbidities in Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder.Biol Psychiatry. 2019 Oct 15;86(8):e25-e27. doi: 10.1016/j.biopsych.2019.08.012. Biol Psychiatry. 2019. PMID: 31558223 No abstract available.
Similar articles
-
Gender differences in psychiatric comorbidity: a population-based study of 40 000 adults with attention deficit hyperactivity disorder.Acta Psychiatr Scand. 2018 Mar;137(3):176-186. doi: 10.1111/acps.12845. Epub 2017 Dec 21. Acta Psychiatr Scand. 2018. PMID: 29266167 Free PMC article.
-
Psychiatric Comorbidities and Psychotropic Medication Use in Autism: A Matched Cohort Study with ADHD and General Population Comparator Groups in the United Kingdom.Autism Res. 2018 Dec;11(12):1690-1700. doi: 10.1002/aur.2040. Epub 2018 Oct 31. Autism Res. 2018. PMID: 30380202
-
Lifetime co-occurring psychiatric disorders in newly diagnosed adults with attention deficit hyperactivity disorder (ADHD) or/and autism spectrum disorder (ASD).BMC Psychiatry. 2020 Aug 26;20(1):423. doi: 10.1186/s12888-020-02828-1. BMC Psychiatry. 2020. PMID: 32847520 Free PMC article.
-
A systematic review of comorbidity between cerebral palsy, autism spectrum disorders and Attention Deficit Hyperactivity Disorder.Eur J Paediatr Neurol. 2019 Jan;23(1):31-42. doi: 10.1016/j.ejpn.2018.10.005. Epub 2018 Nov 2. Eur J Paediatr Neurol. 2019. PMID: 30446273
-
[Comorbidity of autism spectrum disorder and attention deficit with hyperactivity. A review study].Rev Neurol. 2015 Feb 25;60 Suppl 1:S37-43. Rev Neurol. 2015. PMID: 25726822 Review. Spanish.
Cited by
-
Comparative meta-analyses of brain structural and functional abnormalities during cognitive control in attention-deficit/hyperactivity disorder and autism spectrum disorder.Psychol Med. 2020 Apr;50(6):894-919. doi: 10.1017/S0033291720000574. Epub 2020 Mar 27. Psychol Med. 2020. PMID: 32216846 Free PMC article.
-
Understanding the Diversity of Pharmacotherapeutic Management of ADHD With Co-occurring Autism: An Australian Cross-Sectional Survey.Front Psychiatry. 2022 Jun 27;13:914668. doi: 10.3389/fpsyt.2022.914668. eCollection 2022. Front Psychiatry. 2022. PMID: 35832595 Free PMC article.
-
The contribution of copy number variants to psychiatric symptoms and cognitive ability.Mol Psychiatry. 2023 Apr;28(4):1480-1493. doi: 10.1038/s41380-023-01978-4. Epub 2023 Feb 3. Mol Psychiatry. 2023. PMID: 36737482 Free PMC article. Review.
-
COVID-19 and Perceived Changes to Quality of Life, Anxiety, Depression, and Loneliness in Autistic and Other Neurodivergent U.K. Adults.Autism Adulthood. 2022 Sep 1;4(3):233-246. doi: 10.1089/aut.2021.0078. Epub 2022 Aug 31. Autism Adulthood. 2022. PMID: 36606155 Free PMC article.
-
Do psychiatric diseases follow annual cyclic seasonality?PLoS Biol. 2021 Jul 19;19(7):e3001347. doi: 10.1371/journal.pbio.3001347. eCollection 2021 Jul. PLoS Biol. 2021. PMID: 34280189 Free PMC article.
References
-
- Baxter AJ, Brugha TS, Erskine HE, Scheurer RW, Vos T, Scott JG (2015): The epidemiology and global burden of autism spectrum disorders. Psychol Med 45:601–613. - PubMed
-
- Tick B, Colvert E, McEwen F, Stewart C, Woodhouse E, Gillan N, et al. (2016): Autism spectrum disorders and other mental health problems: Exploring etiological overlaps and phenotypic causal associations. J Am Acad Child Adolesc Psychiatry 55:106–113 e104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
