

Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia
- PMID: 31182334
- PMCID: PMC8369495
- DOI: 10.1016/j.ejvs.2019.05.006
Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia
Erratum in
-
Corrigendum to 'Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia' [European Journal of Vascular & Endovascular Surgery 58/1S (2019) 1-109].Eur J Vasc Endovasc Surg. 2020 Mar;59(3):492-493. doi: 10.1016/j.ejvs.2019.11.025. Epub 2019 Dec 10. Eur J Vasc Endovasc Surg. 2020. PMID: 31836510 No abstract available.
-
Corrigendum to "Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischaemia" [Eur J Vasc Endovasc Surg 58 (1S) (2019) 1-109>].Eur J Vasc Endovasc Surg. 2020 Jul;60(1):158-159. doi: 10.1016/j.ejvs.2020.04.033. Eur J Vasc Endovasc Surg. 2020. PMID: 32622518 No abstract available.
Abstract
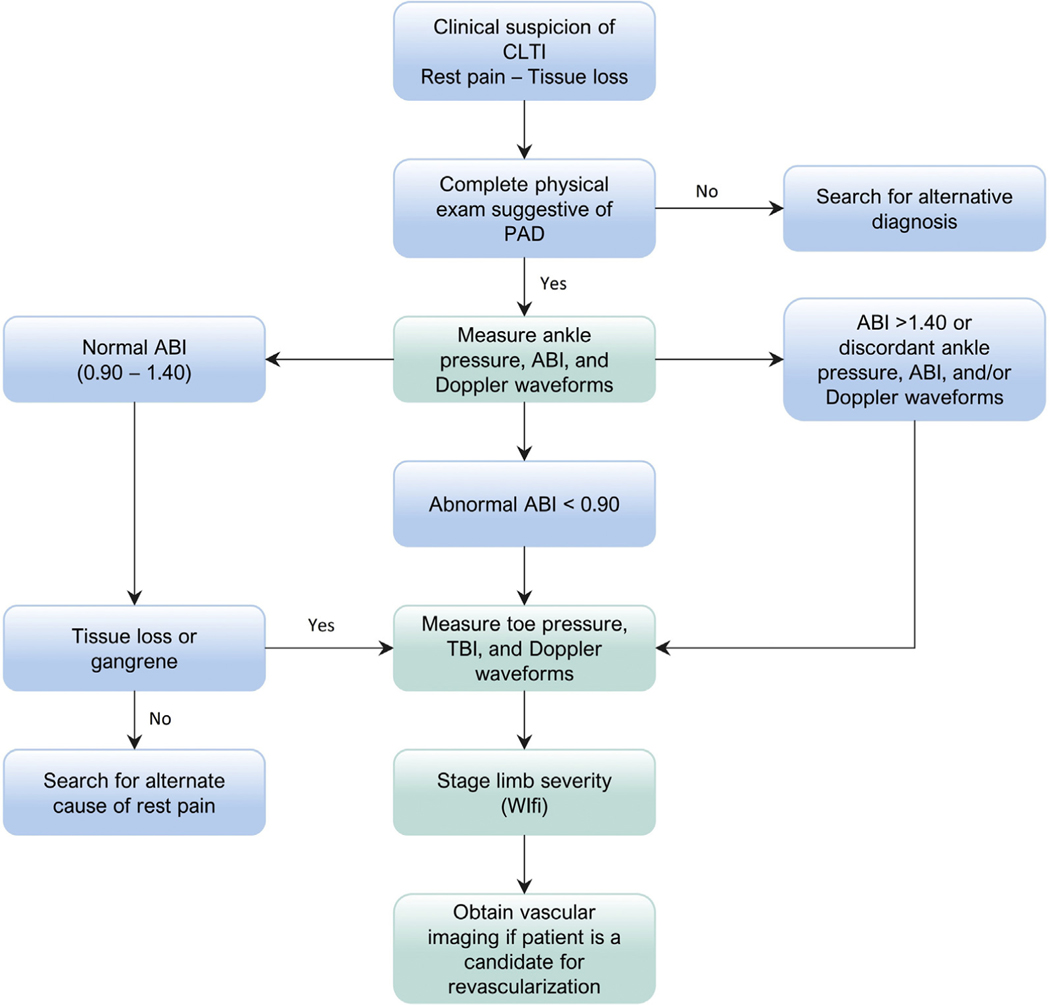
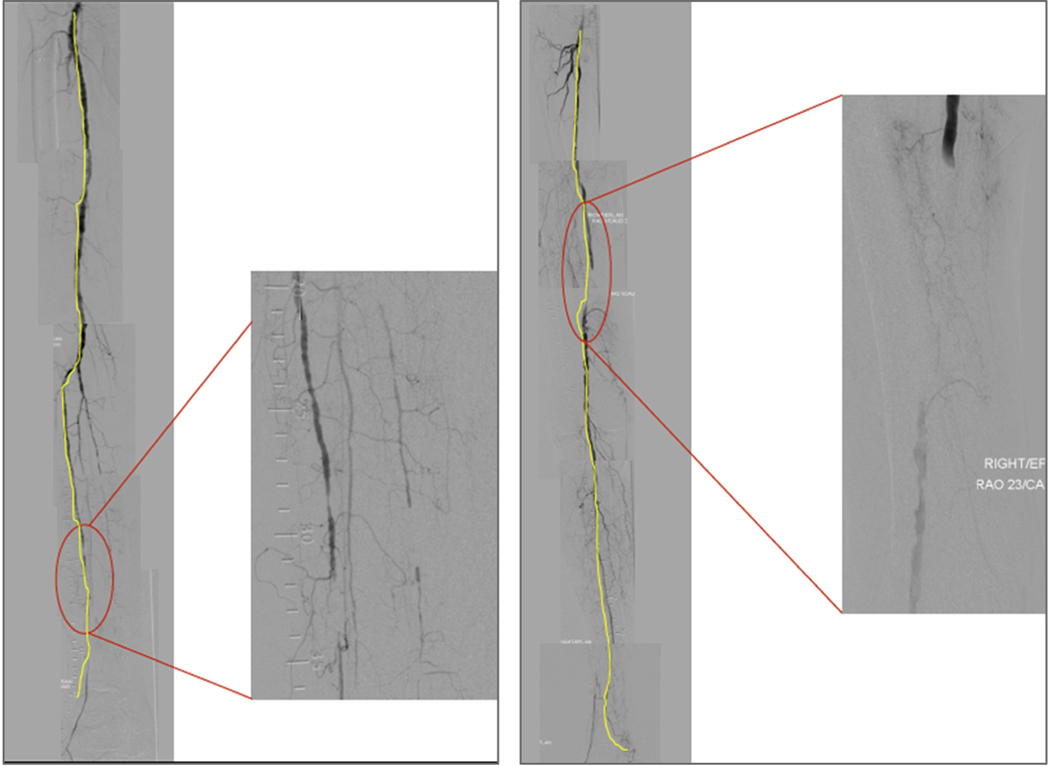
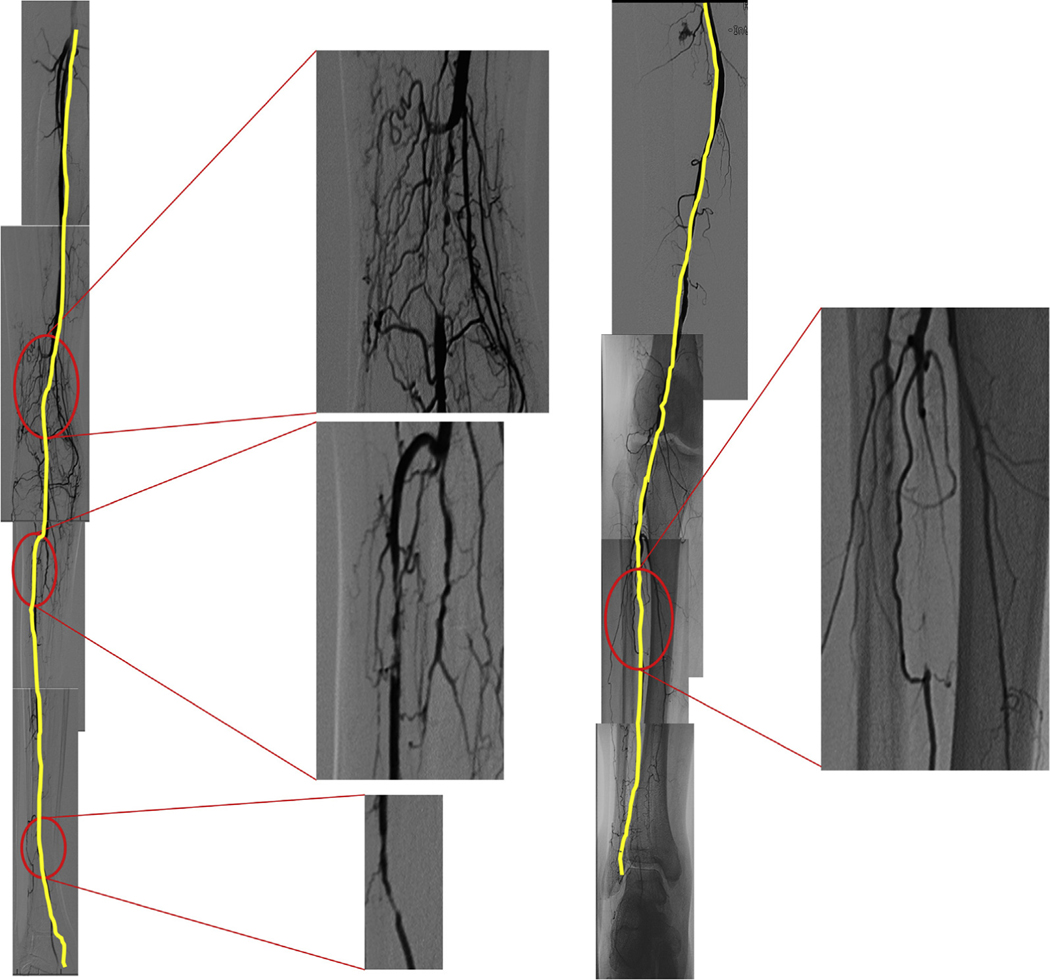
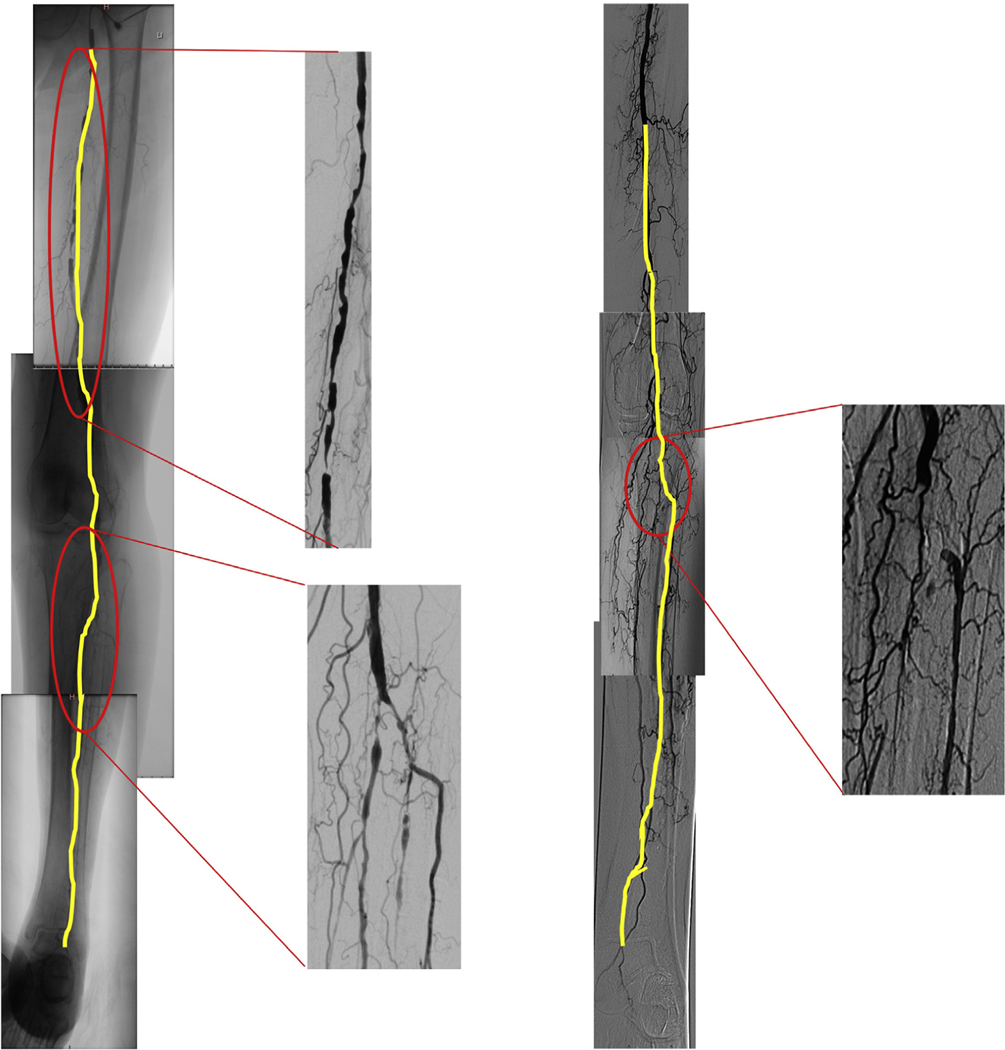
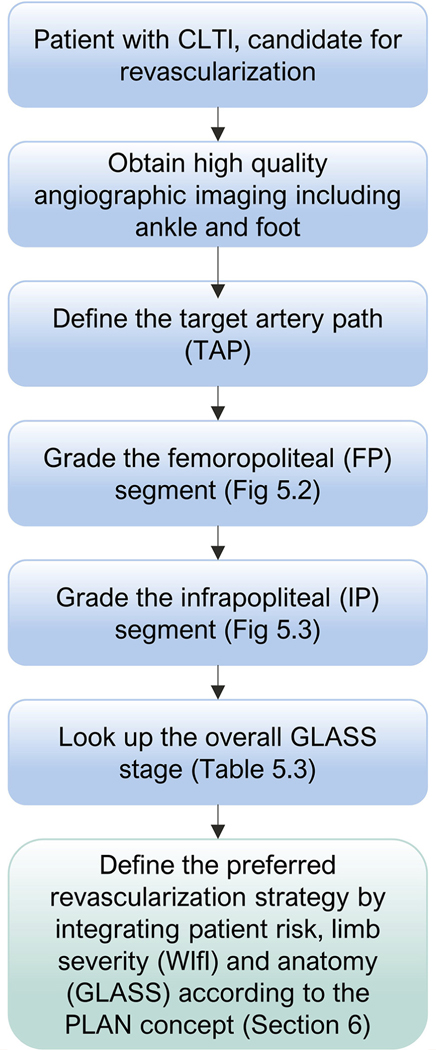
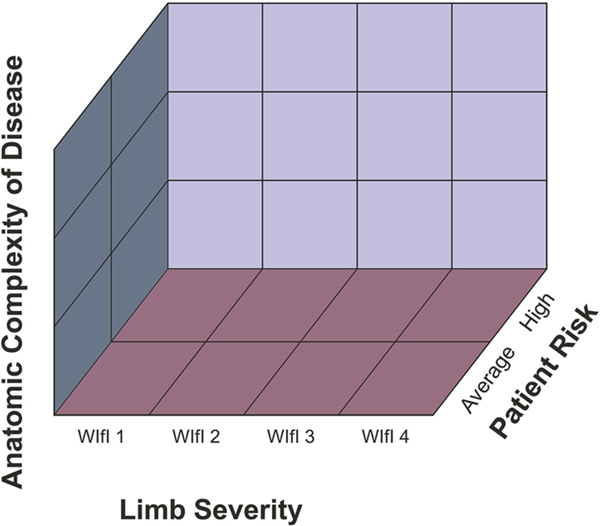
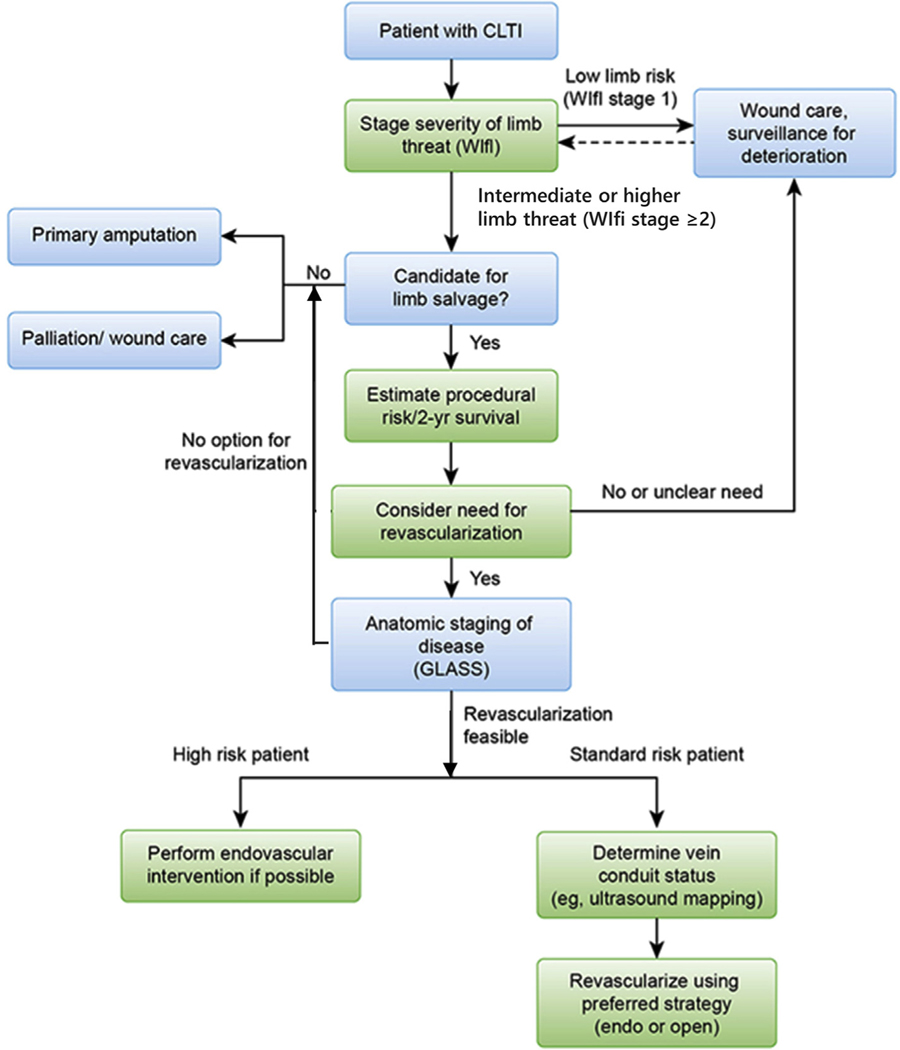
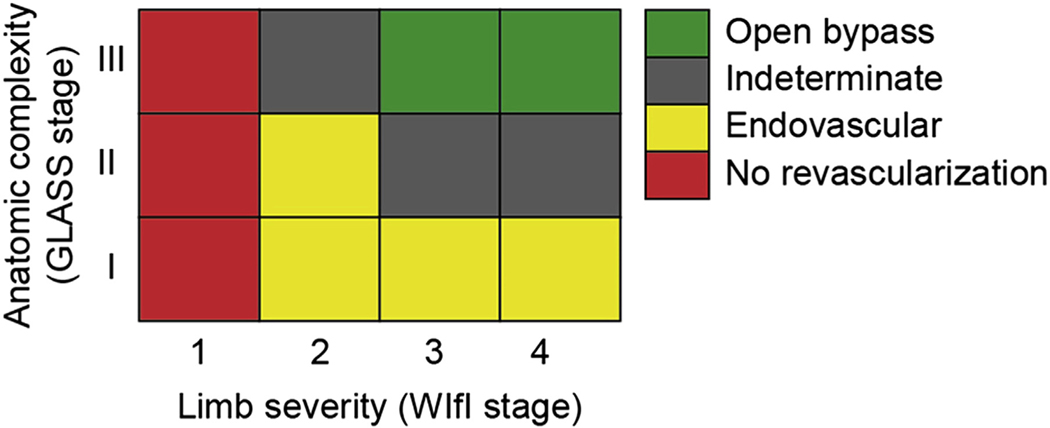
Chronic limb-threatening ischemia (CLTI) is associated with mortality, amputation, and impaired quality of life. These Global Vascular Guidelines (GVG) are focused on definition, evaluation, and management of CLTI with the goals of improving evidence-based care and highlighting critical research needs. The term CLTI is preferred over critical limb ischemia, as the latter implies threshold values of impaired perfusion rather than a continuum. CLTI is a clinical syndrome defined by the presence of peripheral artery disease (PAD) in combination with rest pain, gangrene, or a lower limb ulceration >2 weeks duration. Venous, traumatic, embolic, and nonatherosclerotic etiologies are excluded. All patients with suspected CLTI should be referred urgently to a vascular specialist. Accurately staging the severity of limb threat is fundamental, and the Society for Vascular Surgery Threatened Limb Classification system, based on grading of Wounds, Ischemia, and foot Infection (WIfI) is endorsed. Objective hemodynamic testing, including toe pressures as the preferred measure, is required to assess CLTI. Evidence-based revascularization (EBR) hinges on three independent axes: Patient risk, Limb severity, and ANatomic complexity (PLAN). Average-risk and high-risk patients are defined by estimated procedural and 2-year all-cause mortality. The GVG proposes a new Global Anatomic Staging System (GLASS), which involves defining a preferred target artery path (TAP) and then estimating limb-based patency (LBP), resulting in three stages of complexity for intervention. The optimal revascularization strategy is also influenced by the availability of autogenous vein for open bypass surgery. Recommendations for EBR are based on best available data, pending level 1 evidence from ongoing trials. Vein bypass may be preferred for average-risk patients with advanced limb threat and high complexity disease, while those with less complex anatomy, intermediate severity limb threat, or high patient risk may be favored for endovascular intervention. All patients with CLTI should be afforded best medical therapy including the use of antithrombotic, lipid-lowering, antihypertensive, and glycemic control agents, as well as counseling on smoking cessation, diet, exercise, and preventive foot care. Following EBR, long-term limb surveillance is advised. The effectiveness of nonrevascularization therapies (eg, spinal stimulation, pneumatic compression, prostanoids, and hyperbaric oxygen) has not been established. Regenerative medicine approaches (eg, cell, gene therapies) for CLTI should be restricted to rigorously conducted randomizsed clinical trials. The GVG promotes standardization of study designs and end points for clinical trials in CLTI. The importance of multidisciplinary teams and centers of excellence for amputation prevention is stressed as a key health system initiative.
Keywords: Bypass surgery; Chronic limb-threatening ischemia; Critical limb ischemia; Diabetes; Endovascular intervention; Evidence-based medicine; Foot ulcer; Peripheral artery disease; Practice guideline.
Copyright © 2019 European Society for Vascular Surgery. Published by Elsevier B.V. All rights reserved.
Figures


Comment in
-
Building a global alliance in vascular surgery.J Vasc Surg. 2019 Sep;70(3):663-664. doi: 10.1016/j.jvs.2019.06.178. J Vasc Surg. 2019. PMID: 31445647 No abstract available.
References
-
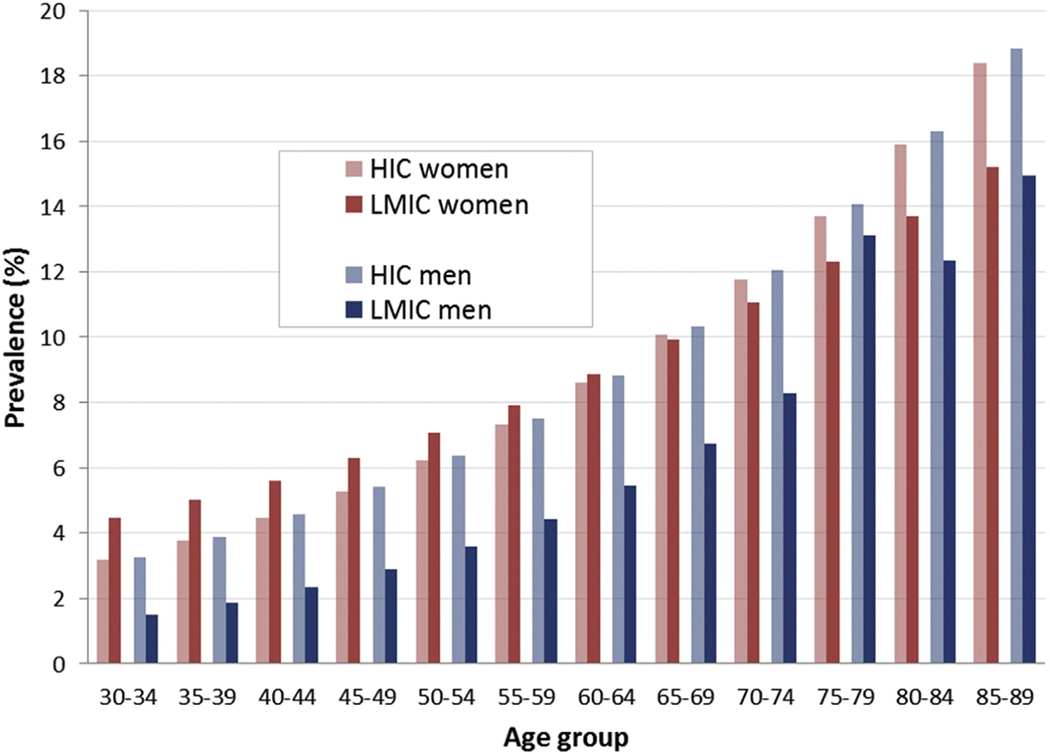
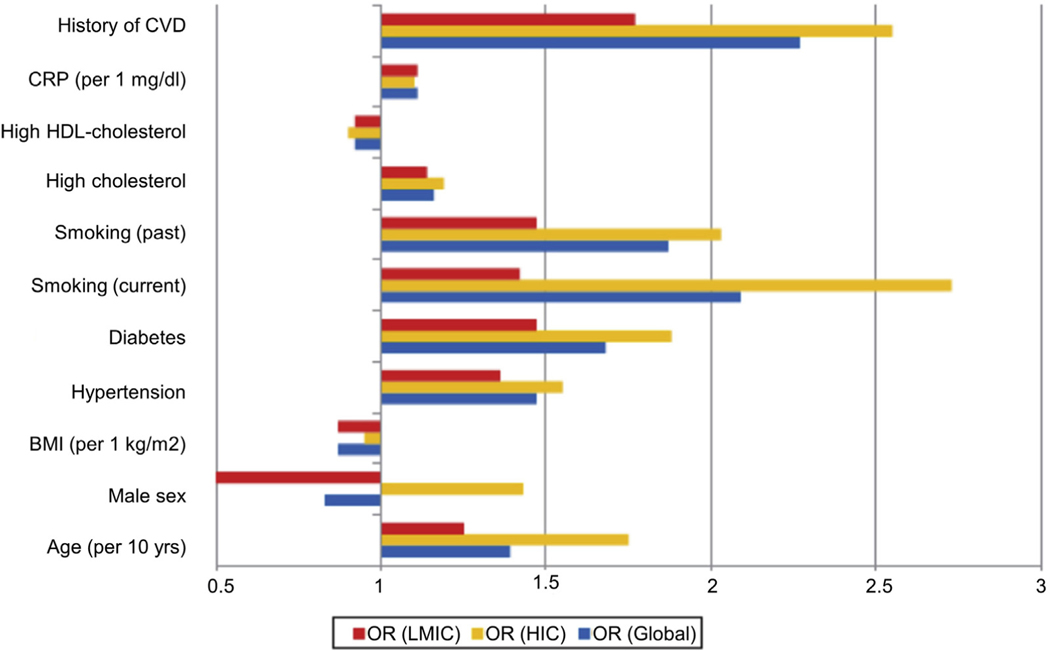
- Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 2013;382:1329–40. - PubMed
-
- Abu Dabrh AM, Steffen MW, Asi N, Undavalli C, Wang Z, Elamin MB, et al. Nonrevascularization-based treatments in patients with severe or critical limb ischemia. J Vasc Surg 2015;62:1330–9.e13. - PubMed
-
- Abu Dabrh AM, Steffen MW, Undavalli C, Asi N, Wang Z, Elamin MB, et al. The natural history of untreated severe or critical limb ischemia. J Vasc Surg 2015;62:1642–51.e3. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
