

The impact of pediatric emergency department crowding on patient and health care system outcomes: a multicentre cohort study
- PMID: 31182457
- PMCID: PMC6565395
- DOI: 10.1503/cmaj.181426
The impact of pediatric emergency department crowding on patient and health care system outcomes: a multicentre cohort study
Abstract
Background: Emergency department overcrowding has been associated with increased odds of hospital admission and mortality after discharge from the emergency department in predominantly adult cohorts. The objective of this study was to evaluate the association between crowding and the odds of several adverse outcomes among children seen at a pediatric emergency department.
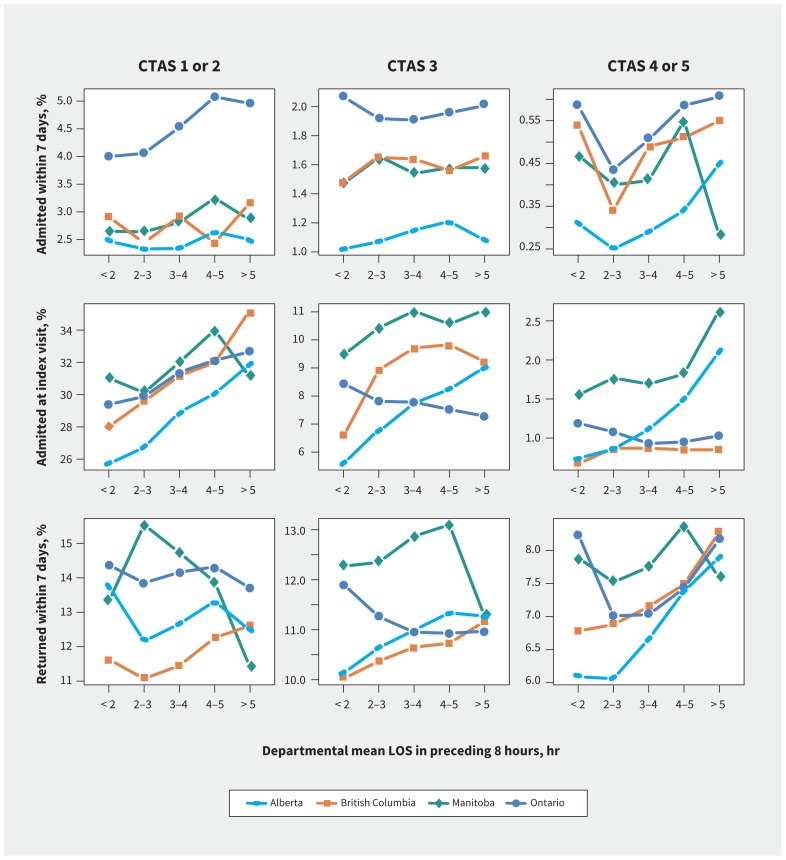
Methods: We conducted a retrospective cohort study involving all children visiting 8 Canadian pediatric emergency departments across 4 provinces between 2010 and 2014. We analyzed the association between mean departmental length of stay for each index visit and hospital admission within 7 days or death within 14 days of emergency department discharge, as well as hospital admission at index visit and return visits within 7 days, using mixed-effects logistic regression modelling.
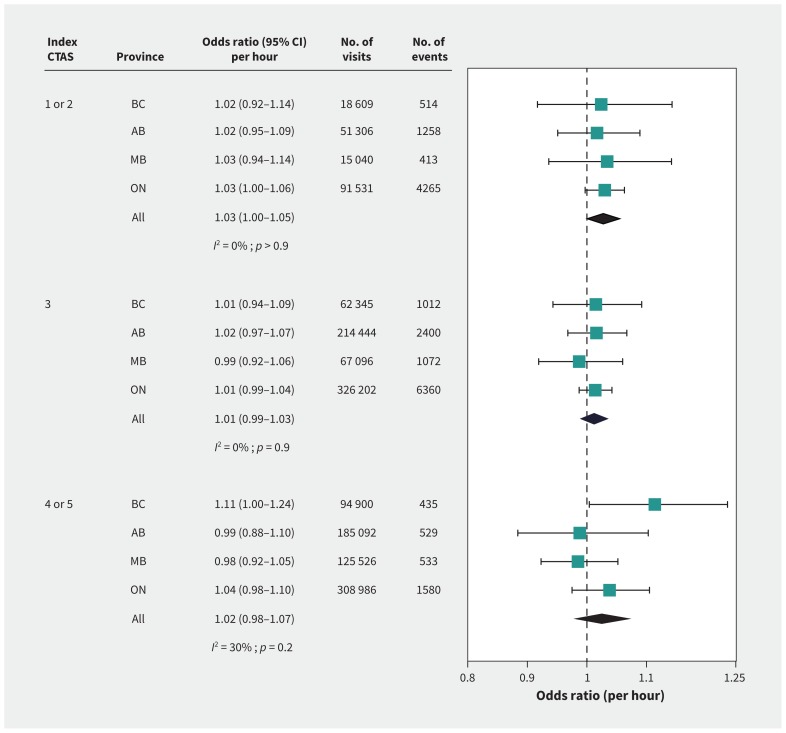
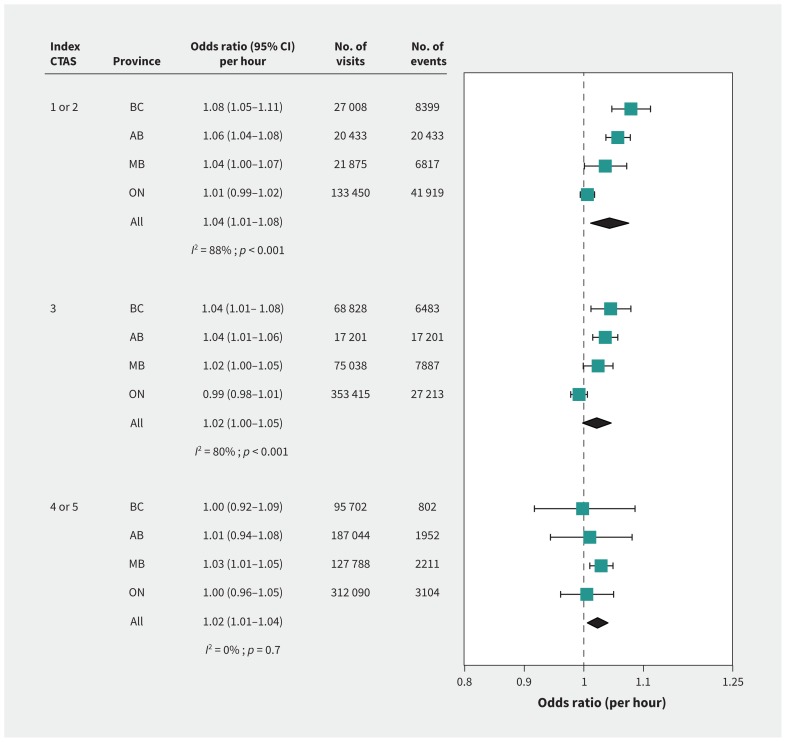
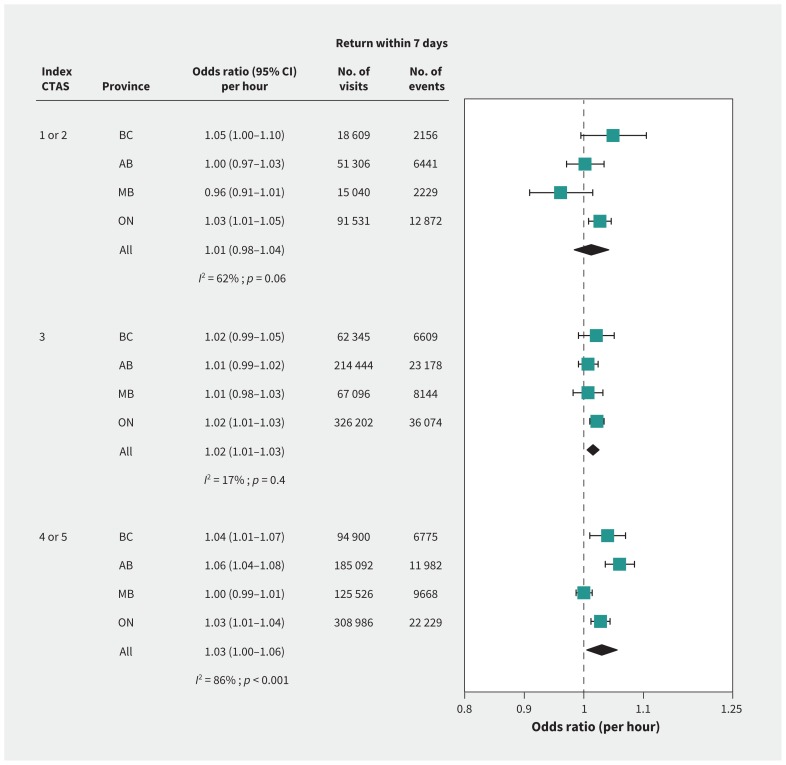
Results: A total of 1 931 465 index visits occurred across study sites over the 5-year period, with little variation in index visit hospital admission or median length of stay. Hospital admission within 7 days of discharge and 14-day mortality were low across provinces (0.8%-1.5% and < 10 per 100 000 visits, respectively), and their association with mean departmental length of stay varied by triage categories and across sites but was not significant. There were increased odds of hospital admission at the index visit with increasing departmental crowding among visits triaged to Canadian Triage and Acuity Scale (CTAS) score 1-2 (odds ratios [ORs] ranged from 1.01 to 1.08) and return visits among patients with a CTAS score of 4-5 discharged at the index visit at some sites (ORs ranged from 1.00 to 1.06).
Interpretation: Emergency department crowding was not significantly associated with hospital admission within 7 days of the emergency department visit or mortality in children. However, it was associated with increased hospital admission at the index visit for the sickest children, and with return visits to the emergency department for those less sick.
© 2019 Joule Inc. or its licensors or its licensors.
Conflict of interest statement
Competing interests: Quynh Doan reports a Scholars Award from the Michael Smith Foundation for Health Research during the conduct of the study. No other competing interests were declared.
Figures
Comment in
-
Demand, overcrowding and the pediatric emergency department.CMAJ. 2019 Jun 10;191(23):E625-E626. doi: 10.1503/cmaj.190610. Epub 2019 Jun 10. CMAJ. 2019. PMID: 32392478 Free PMC article. No abstract available.
References
-
- Affleck A, Parks P, Drummond A, et al. Emergency department overcrowding and access block. CJEM 2013;15:359–84. - PubMed
-
- Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust 2006;184:213–6. - PubMed
-
- Rondeau KV, Francescutti LH. Emergency department overcrowding: the impact of resource scarcity on physician job satisfaction. J Healthc Manag 2005; 50:327–40. - PubMed
-
- Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med 2009;16:1–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources