

HIV infection and coronary heart disease: mechanisms and management
- PMID: 31182833
- PMCID: PMC8015945
- DOI: 10.1038/s41569-019-0219-9
HIV infection and coronary heart disease: mechanisms and management
Abstract
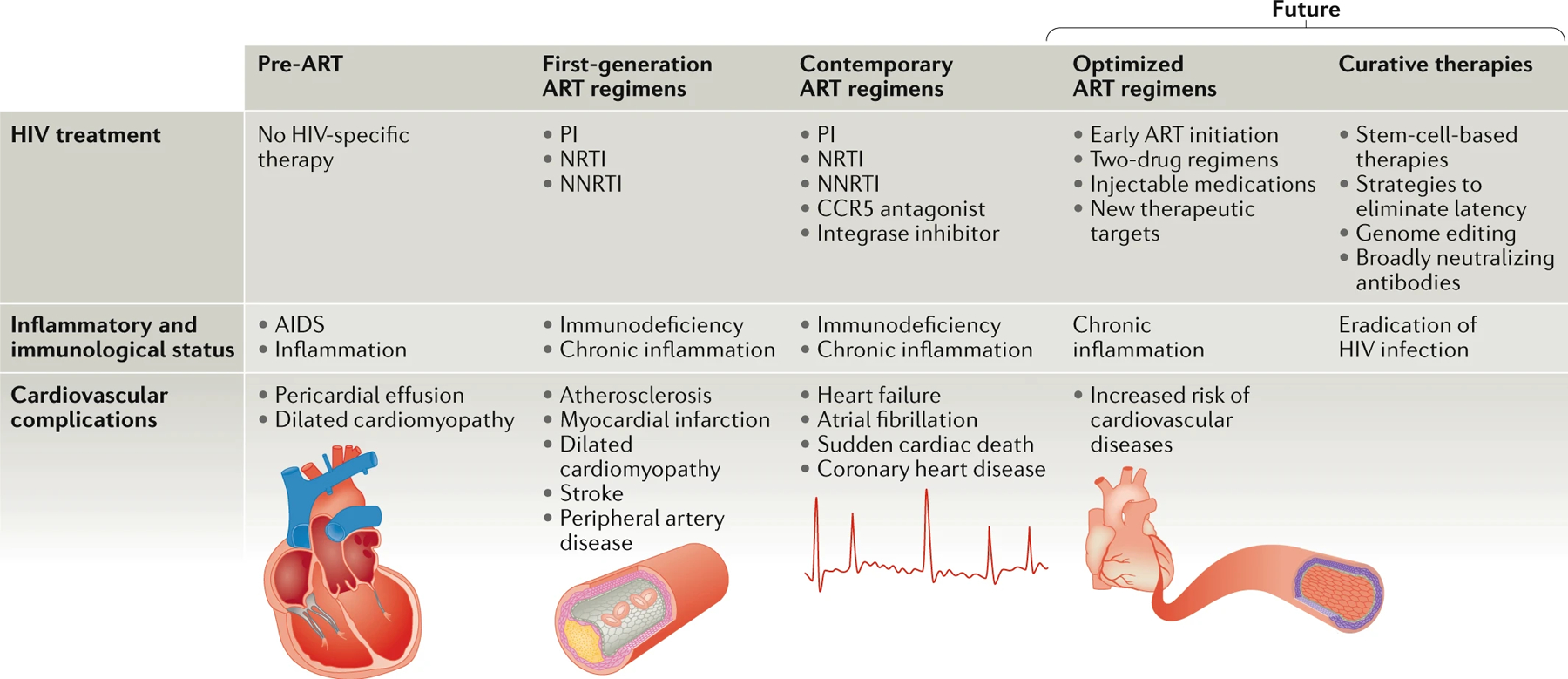
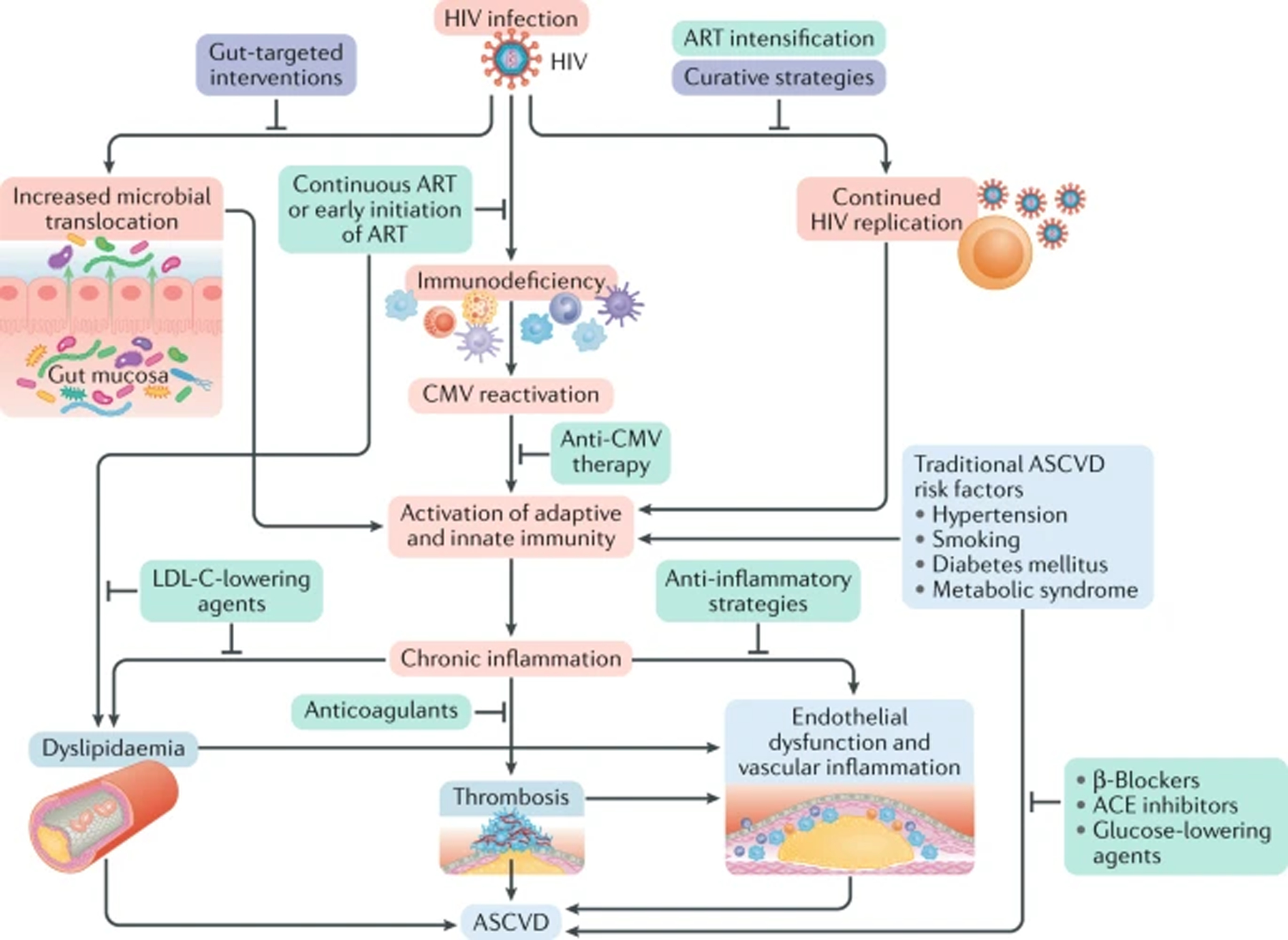
Antiretroviral therapy has largely transformed HIV infection into a chronic disease condition. As such, physicians and other providers caring for individuals living with HIV infection need to be aware of the potential cardiovascular complications of HIV infection and the nuances of how HIV infection increases the risk of cardiovascular diseases, including acute myocardial infarction, stroke, peripheral artery disease, heart failure and sudden cardiac death, as well as how to select available therapies to reduce this risk. In this Review, we discuss the epidemiology and clinical features of cardiovascular disease, with a focus on coronary heart disease, in the setting of HIV infection, which includes a substantially increased risk of myocardial infarction even when the HIV infection is well controlled. We also discuss the mechanisms underlying HIV-associated atherosclerotic cardiovascular disease, such as the high rates of traditional cardiovascular risk factors in patients with HIV infection and HIV-related factors, including the use of antiretroviral therapy and chronic inflammation in the setting of effectively treated HIV infection. Finally, we highlight available therapeutic strategies, as well as approaches under investigation, to reduce the risk of cardiovascular disease and lower inflammation in patients with HIV infection.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Redfield MM Heart failure with preserved ejection fraction. N. Engl. J. Med 375, 1868–1877 (2016). - PubMed
