

Long-Term Survival, Quality of Life, and Psychosocial Outcomes in Advanced Melanoma Patients Treated with Immune Checkpoint Inhibitors
- PMID: 31182961
- PMCID: PMC6512024
- DOI: 10.1155/2019/5269062
Long-Term Survival, Quality of Life, and Psychosocial Outcomes in Advanced Melanoma Patients Treated with Immune Checkpoint Inhibitors
Abstract
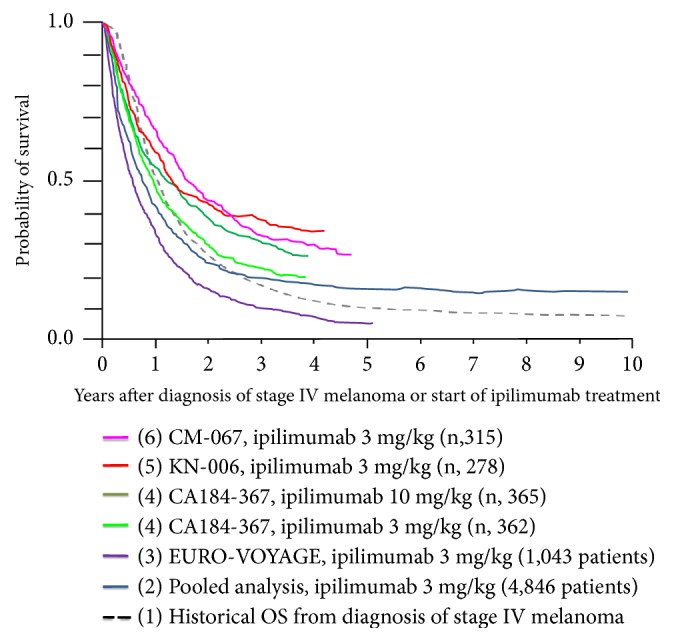
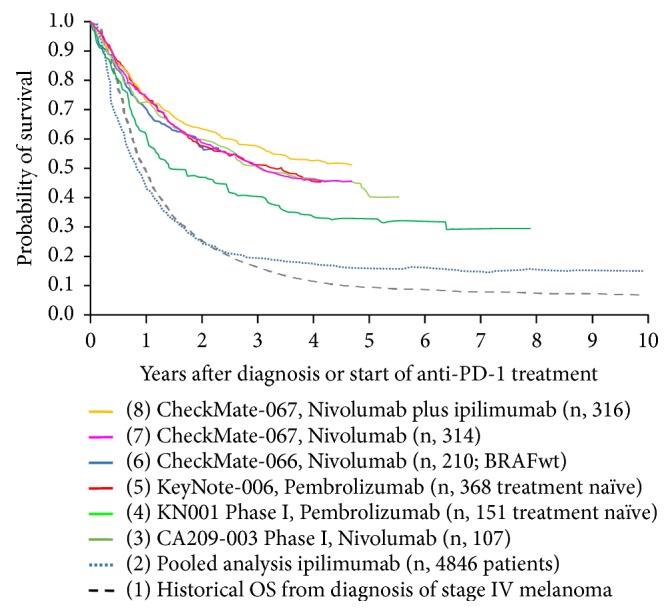
Immune checkpoint inhibitors have become a standard of care option for the treatment of patients with advanced melanoma. Since the approval of the first immune checkpoint (CTLA-4) inhibitor ipilimumab in 2011 and programmed death-1 (PD-1) blocking monoclonal antibodies pembrolizumab and nivolumab thereafter, an increasing proportion of patients with unresectable advanced melanoma achieved long-term overall survival. Little is known about the psychosocial wellbeing, neurocognitive function, and quality of life (QOL) of these survivors. Knowledge about the long term side-effects of these novel treatments is scarce as long-term survivorship is a novel issue in the field of immunotherapy. The purpose of this review is to summarize our current knowledge regarding the survival and safety results of pivotal clinical trials in the field of advanced melanoma and to highlight potential long-term consequences that are likely to impact psychosocial wellbeing, neurocognitive functioning, and QOL. The issues raised substantiate the need for clinical investigation of these issues with the aim of optimizing comprehensive health care for advanced melanoma survivors.
Figures
References
-
- Atkins M. B., Hsu J., Lee S., et al. Phase III trial comparing concurrent biochemotherapy with cisplatin, vinblastine, dacarbazine, interleukin-2, and interferon alfa-2b with cisplatin, vinblastine, and dacarbazine alone in patients with metastatic malignant melanoma (E3695): a trial coordinated by the Eastern Cooperative Oncology Group. Journal of Clinical Oncology. 2008;26(35):5748–5754. doi: 10.1200/JCO.2008.17.5448. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
