

A Meta-Analysis of Resveratrol Protects against Myocardial Ischemia/Reperfusion Injury: Evidence from Small Animal Studies and Insight into Molecular Mechanisms
- PMID: 31182995
- PMCID: PMC6512035
- DOI: 10.1155/2019/5793867
A Meta-Analysis of Resveratrol Protects against Myocardial Ischemia/Reperfusion Injury: Evidence from Small Animal Studies and Insight into Molecular Mechanisms
Abstract
Aims: Myocardial ischemia/reperfusion (I/R) injury is a leading cause of cardiomyocyte loss and subsequent ventricular dysfunction after restoring the coronary blood flow and contributes to considerable increase in morbidity and mortality. Resveratrol has been declared to confer cardioprotection against in vivo and ex vivo myocardial I/R injury. Here, we have sought to investigate the effects of preconditioning with resveratrol on myocardial I/R damage across the small animal studies.
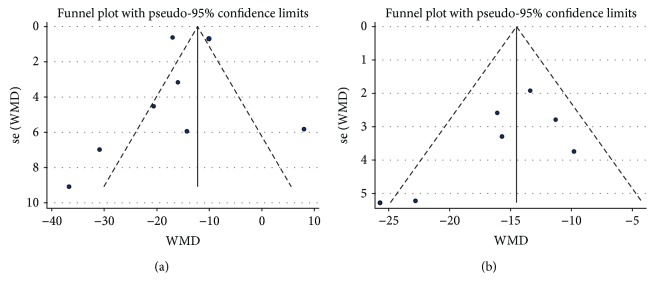
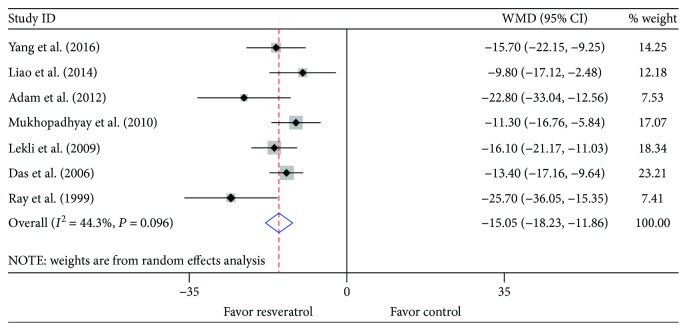
Methods and results: The MEDLINE, Google Scholar, PubMed, and Cochrane databases were searched for preclinical studies investigating resveratrol vs. vehicle published from the inception to July 2018. Eventually, 10 in vivo and 7 ex vivo studies with 261 animals (130 for resveratrol; 131 for vehicle) were included for meta-analysis. Pooled estimates for primary outcomes demonstrated that pretreatment with resveratrol significantly reduced the infarct size after myocardial I/R injury irrespective of in vivo (weighted mean difference (WMD): -13.42, 95% CI: -16.63 to -10.21, P ≤ 0.001) or ex vivo (WMD: -15.05, 95% CI: -18.23 to -11.86, P ≤ 0.001) studies. Consistently, stratified analysis according to the reperfusion duration, route of administration, or timing regimen of pretreatment all showed the infarct-sparing benefit of resveratrol. Metaregression did not indicate any difference in infarct size based on species, sample size, state, route of administration, reperfusion duration, and timing regimen of pretreatment. Meanwhile, sensitivity analysis also identified the cardioprotection of resveratrol with robust results in spite of significant heterogeneity.
Conclusions: Preconditioning with resveratrol appears to prevent the heart from I/R injury in comparison with vehicle, as evidenced by limited infarct size in a preclinical setting. Studies with large animals or randomized controlled trials will add more evidence and provide the rationale for clinical use.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
