

Adrenal glands hemorrhages: embolization in acute setting
- PMID: 31183321
- PMCID: PMC6534759
- DOI: 10.21037/gs.2018.10.06
Adrenal glands hemorrhages: embolization in acute setting
Abstract
Background: Acute adrenal hemorrhages are a rare event compared to other abdominal visceral injuries because of the anatomic localization of the adrenal glands; main causes are trauma and ruptured neoplasms. This manuscript reports on a single center experience of transarterial embolizations of adrenal hemorrhages in emergency setting.
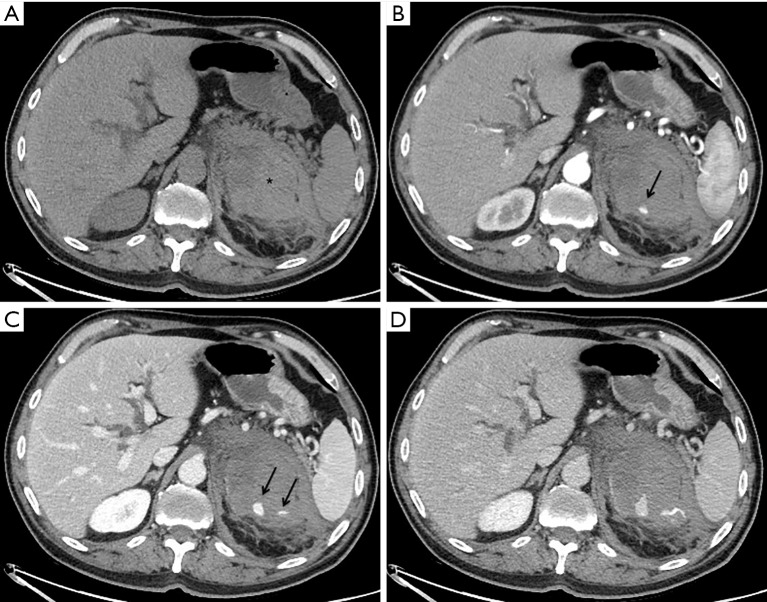
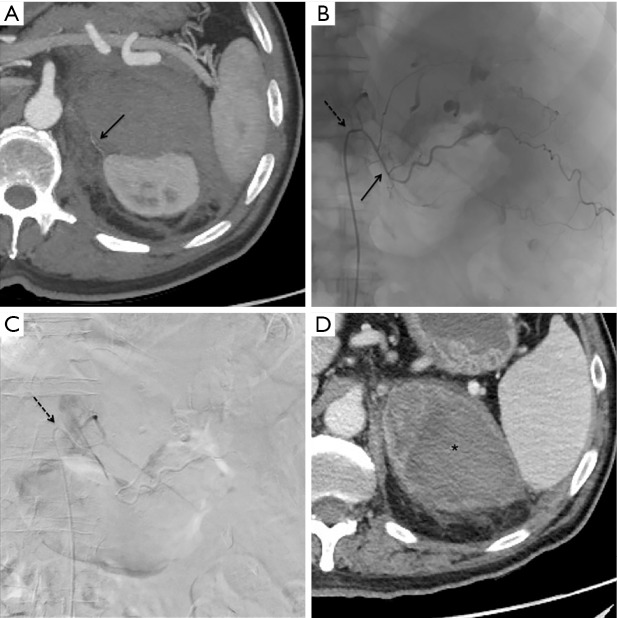
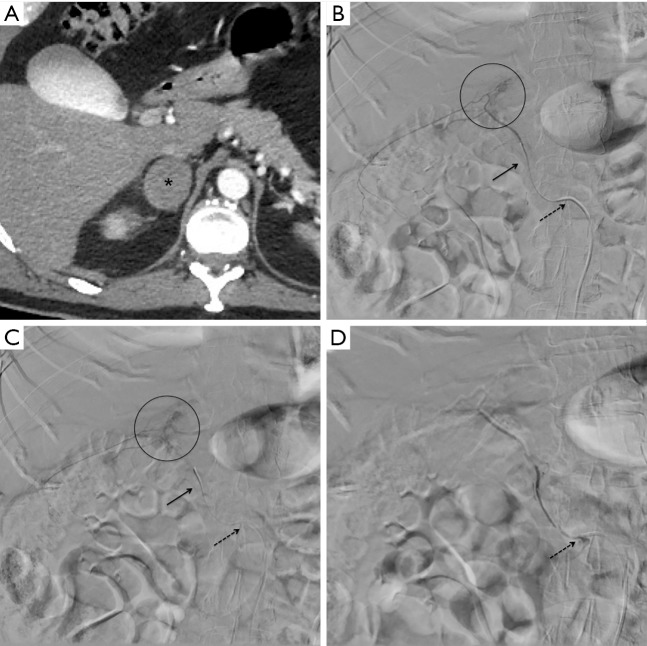
Methods: In this retrospective analysis from 2010 to date, 17 patients (12 men and 5 women, mean age: 59.8 years) presenting with adrenal bleedings were treated by endovascular embolization. The etiology was traumatic in 7 cases, ruptured neoplasm in 8 cases and spontaneous in 2 patients assuming oral anticoagulant therapy. After thin slice contrast enhanced CT, a superselective embolization was conducted with different embolizing agents according to the type of vessel lesion and operator preference.
Results: Technical success rate, considered as interruption of adrenal bleeding detectable at angiography, was 94.1%. Clinical success rate, considered as hemodynamic stability restoration within 24 hours from the procedure, was 82.3%. Vessels involved were the superior adrenal artery in 5 patients, the middle adrenal artery in 8 patients, the inferior adrenal artery in one patient and more than one adrenal artery in 3 patients. No procedure-related major complications occurred and no patients had infarctions, necrosis, abscess formation, or required long-term steroid supplementation.
Conclusions: Acute adrenal hemorrhages can be safely and effectively managed by catheter directed embolizations; the source of bleeding has to be carefully investigated at CT and angiography because adrenal glands present with a wide and complex vascular arterial network.
Keywords: Adrenal gland; acute; embolization; hemorrhage.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Spontaneous hemorrhage of an adrenal myelolipoma treated with transarterial embolization: A case report.Radiol Case Rep. 2020 May 7;15(7):961-965. doi: 10.1016/j.radcr.2020.04.034. eCollection 2020 Jul. Radiol Case Rep. 2020. PMID: 32419895 Free PMC article.
-
Post-Traumatic Intraparenchymal Renal Hemorrhages: Correlation between CT and DSA Vascular Findings for Superselective Embolization Procedures.Diagnostics (Basel). 2021 Jul 14;11(7):1256. doi: 10.3390/diagnostics11071256. Diagnostics (Basel). 2021. PMID: 34359339 Free PMC article.
-
Combined DSA- and US-guided management of acute bleeding: effectiveness of percutaneous glue embolization in six cases.J Ultrasound. 2024 Mar;27(1):179-184. doi: 10.1007/s40477-023-00785-5. Epub 2023 May 10. J Ultrasound. 2024. PMID: 37162728 Free PMC article.
-
The role of interventional radiology in hepatic and renal hemorrhage embolization: single center experience and literature review.Acta Biomed. 2021 Sep 10;92(S5):e2021405. doi: 10.23750/abm.v92iS5.11876. Acta Biomed. 2021. PMID: 34505844 Free PMC article. Review.
-
Endovascular management of internal carotid artery injuries secondary to endonasal surgery: case series and review of the literature.J Neurosurg. 2016 Nov;125(5):1256-1276. doi: 10.3171/2015.6.JNS142483. Epub 2016 Jan 15. J Neurosurg. 2016. PMID: 26771847 Review.
Cited by
-
Approach to the Patient With Adrenal Hemorrhage.J Clin Endocrinol Metab. 2023 Mar 10;108(4):995-1006. doi: 10.1210/clinem/dgac672. J Clin Endocrinol Metab. 2023. PMID: 36404284 Free PMC article.
-
Two cases of atraumatic adrenal hemorrhage: A review of active management, conservative management, and challenges faced.Radiol Case Rep. 2024 Mar 26;19(6):2395-2401. doi: 10.1016/j.radcr.2024.03.005. eCollection 2024 Jun. Radiol Case Rep. 2024. PMID: 38645544 Free PMC article.
-
Adrenal Hemorrhage as a Complication of Plug-assisted Retrograde Transvenous Obliteration of Gastrorenal Shunt Managed by Adrenal Artery Embolization: A Case Report.Interv Radiol (Higashimatsuyama). 2024 Aug 7;9(3):180-185. doi: 10.22575/interventionalradiology.2023-0032. eCollection 2024 Nov 1. Interv Radiol (Higashimatsuyama). 2024. PMID: 39559814 Free PMC article.
-
Retroperitoneal Laparoscopic Surgery in the Treatment of Complex Adrenal Tumors.Cancer Manag Res. 2020 Jul 14;12:5787-5791. doi: 10.2147/CMAR.S257310. eCollection 2020. Cancer Manag Res. 2020. PMID: 32765081 Free PMC article.
-
Spontaneous hemorrhage of an adrenal myelolipoma treated with transarterial embolization: A case report.Radiol Case Rep. 2020 May 7;15(7):961-965. doi: 10.1016/j.radcr.2020.04.034. eCollection 2020 Jul. Radiol Case Rep. 2020. PMID: 32419895 Free PMC article.
References
-
- Ierardi AM, Iacobellis F, Carrafiello G, et al. Vascular Emergencies of the Retroperitoneum: Recent Advances in MDCT and Interventional Radiology. In: Patlas M, Katz D, Scaglione M. editors. 2018 MDCT and MR Imaging of Acute Abdomen. Cham: Springer International Publishing; 2018;151-77.
LinkOut - more resources
Full Text Sources
Medical