

Meta-analysis of postoperative pain using non-sutured or sutured single-layer open mesh repair for inguinal hernia
- PMID: 31183441
- PMCID: PMC6551402
- DOI: 10.1002/bjs5.50139
Meta-analysis of postoperative pain using non-sutured or sutured single-layer open mesh repair for inguinal hernia
Abstract
Background: Chronic postoperative pain occurs in up to 21·7 per cent of patients undergoing open inguinal hernia repair. Several mesh fixation techniques using glue or self-gripping meshes have been developed to reduce postoperative pain. The aim of this meta-analysis was to evaluate RCTs comparing adhesional/self-gripping and sutured single-layer open mesh fixations in the repair of inguinal herniation, with postoperative pain as endpoint.
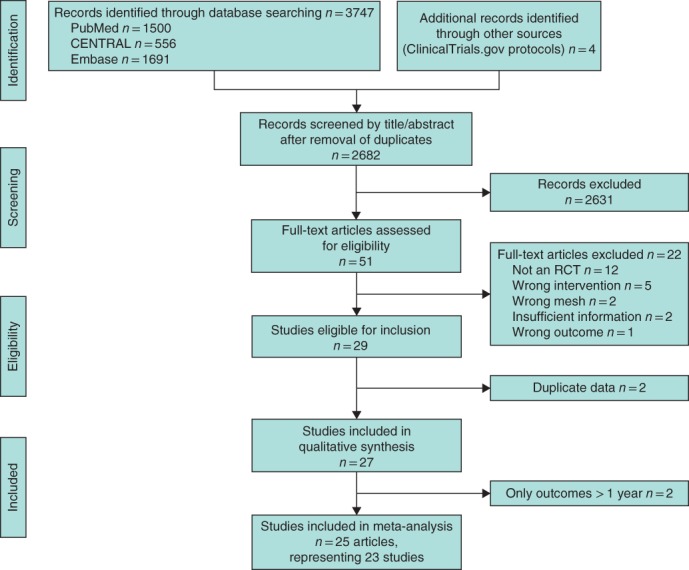
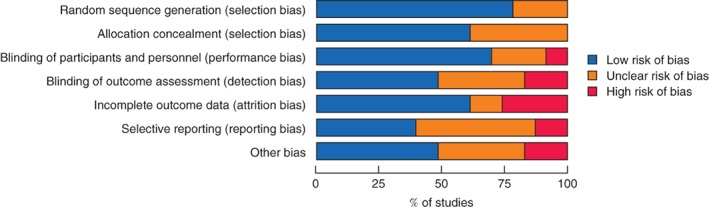
Methods: PubMed, Embase and Cochrane CENTRAL databases were searched systematically for RCTs according to the PRISMA guidelines; the study was registered at PROSPERO (CRD42017056373). Different fixation methods were analysed. The primary outcome, chronic pain, was defined as a postoperative visual analogue scale (VAS) score of at least 3 at 12 months. Secondary outcomes were mean VAS score at 1 week and at 1 month after surgery.
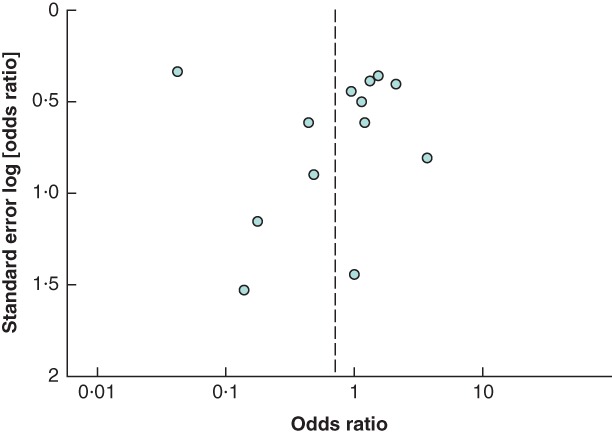
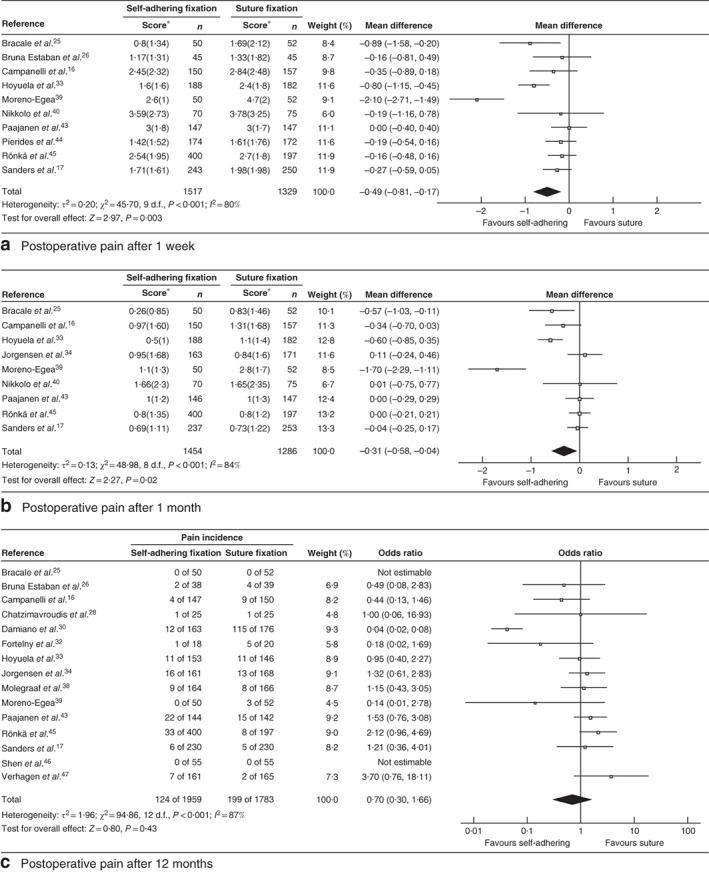
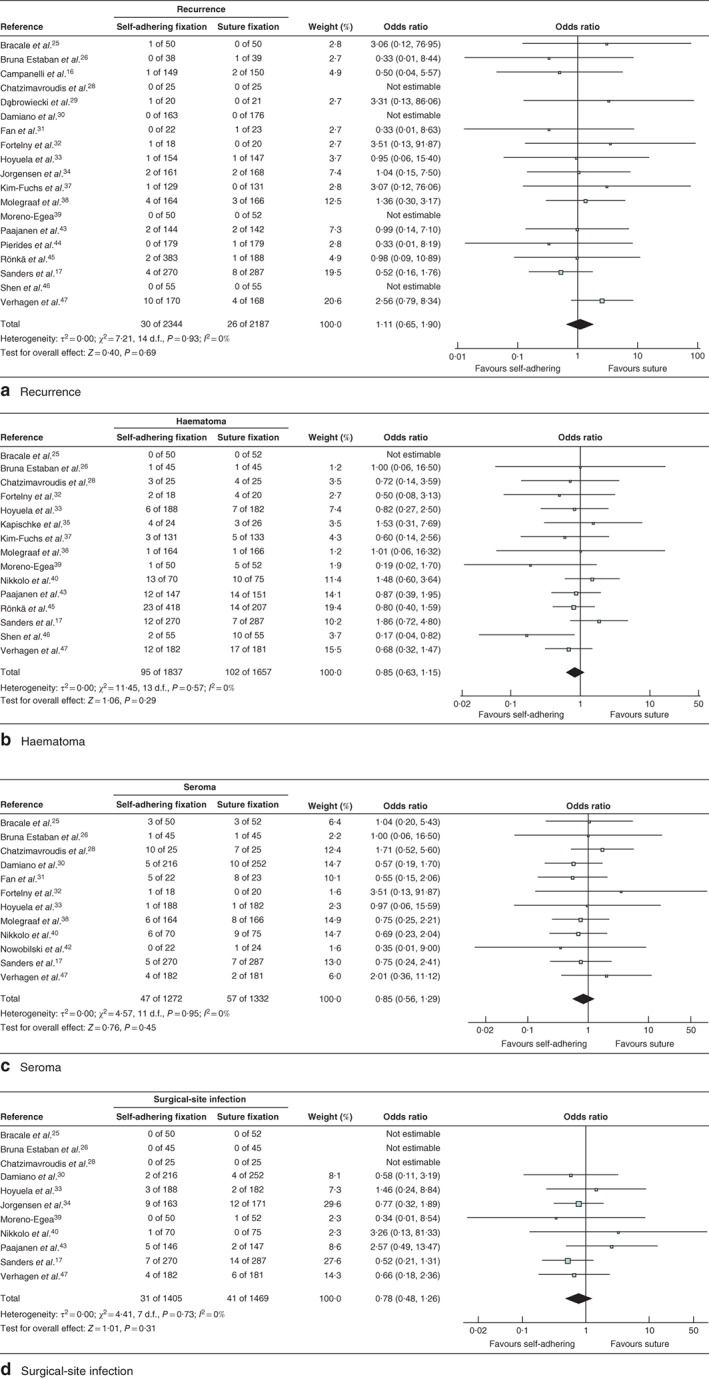
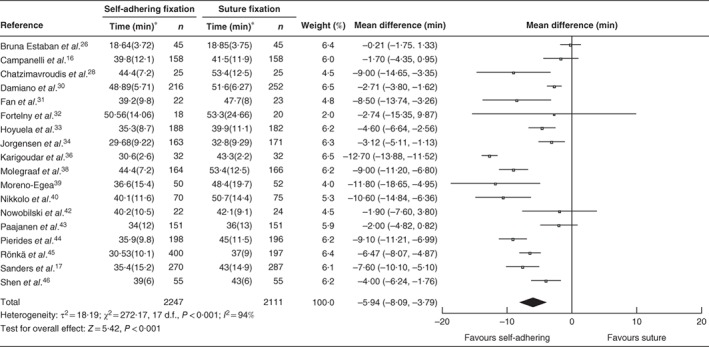
Results: Twenty-three studies including 5190 patients were included in the meta-analysis. Adhesional (self-adhering or glued) or self-gripping fixation methods were associated with a significantly lower VAS score at 1 week (mean difference -0·49, 95 per cent c.i. -0·81 to -0·17; P = 0·003) and at 1 month (mean difference -0·31, -0·58 to -0·04; P = 0·02) after surgery than suture fixation, but the incidence of chronic pain after 12 months was similar in the two groups (odds ratio 0·70, 95 per cent c.i. 0·30 to 1·66). Differences in recurrences and complications between groups did not reach statistical significance.
Conclusion: There was no difference in the incidence of chronic pain 12 months after different mesh repair fixation techniques despite significant reductions in short-term postoperative pain favouring a non-sutured technique. There were no differences in recurrence rates or in rates of other complications at 1 year.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
