

Evaluation of a strategy using pretherapeutic fiducial marker placement to avoid missing liver metastases
- PMID: 31183451
- PMCID: PMC6551408
- DOI: 10.1002/bjs5.50140
Evaluation of a strategy using pretherapeutic fiducial marker placement to avoid missing liver metastases
Abstract
Background: Hepatic surgery is appropriate for selected patients with colorectal liver metastases (CRLM). Advances in chemotherapy have led to modification of management, particularly when metastases disappear. Treatment should address all initial CRLM sites based on pretherapeutic cross-sectional imaging. This study aimed to evaluate pretherapeutic fiducial marker placement to optimize CRLM treatment.
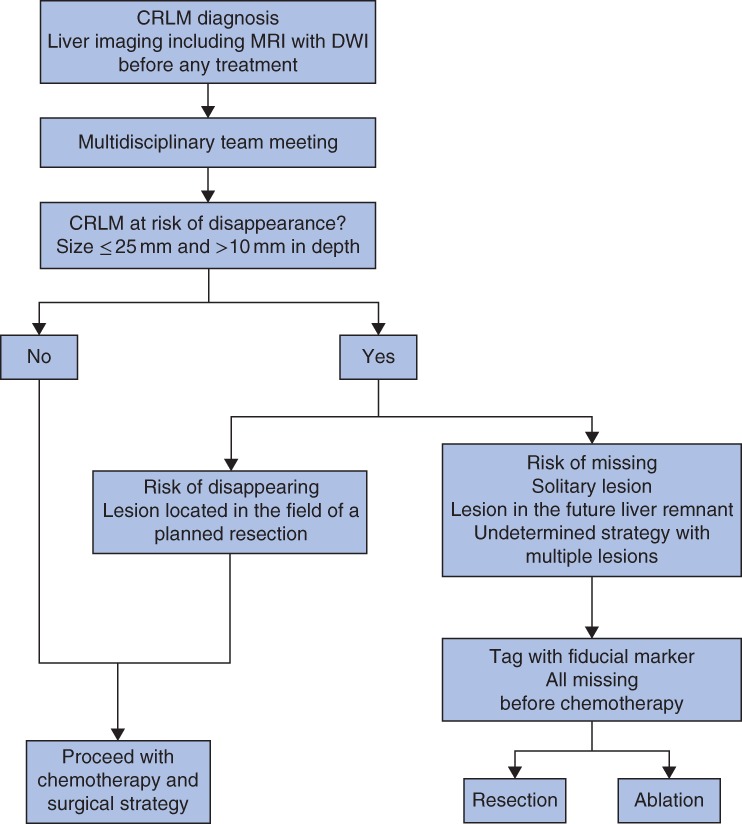
Methods: This pilot investigation included patients with CRLM who were considered for potentially curative treatment between 2009 and 2016. According to a multidisciplinary team decision, lesions smaller than 25 mm in diameter that were more than 10 mm deep in the hepatic parenchyma and located outside the field of a planned resection were marked. Complication rates and clinicopathological data were analysed.
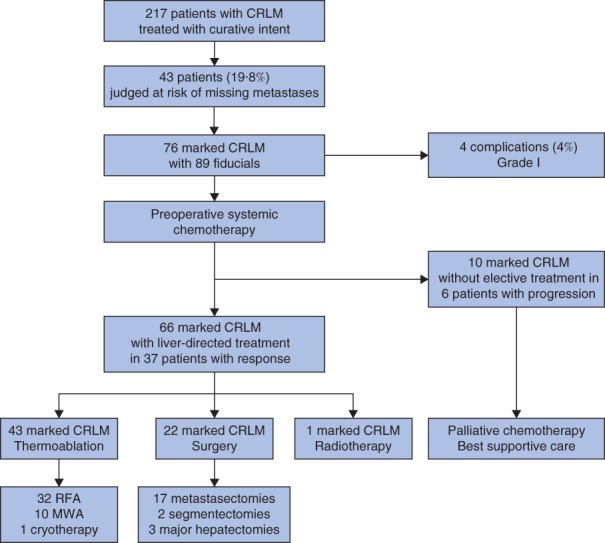
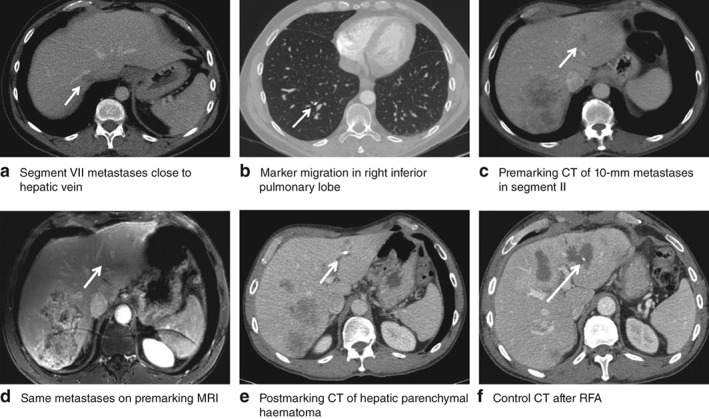
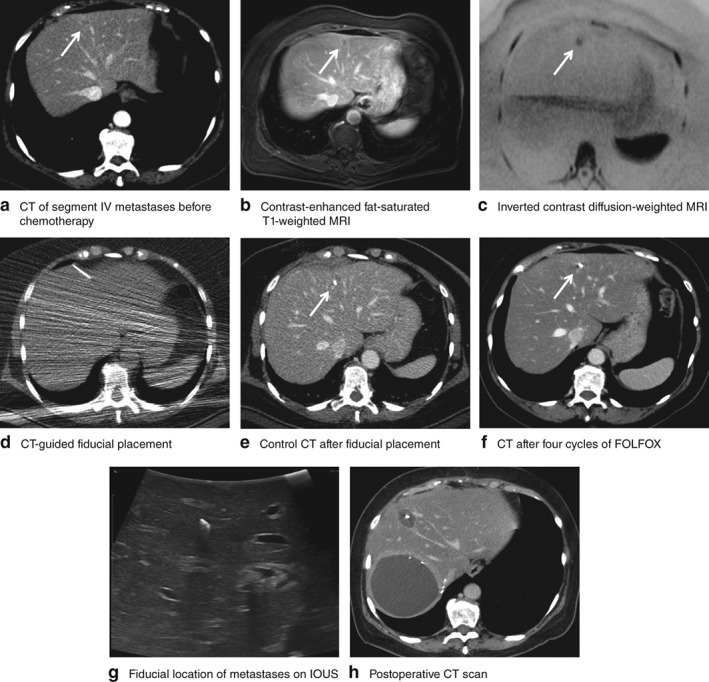
Results: Some 76 metastases were marked in 43 patients among 217 patients with CRLM treated with curative intent. Of these, 23 marked CRLM (30 per cent), with a mean(s.d.) size of 11·0(3·4) mm, disappeared with preoperative chemotherapy. There were four complications associated with marking: two intrahepatic haematomas, one fiducial migration and one misplacement. After a median follow-up of 47·7 (range 18·1-144·9) months, no needle-track seeding was noted. Of four disappearing CRLM that were marked and resected, two presented with persistent active disease. Other missing lesions were treated with thermoablation.
Conclusion: Pretherapeutic fiducial marker placement appears useful for the curative management of CRLM.
Figures
References
-
- Van Cutsem E, Nordlinger B, Adam R, Köhne CH, Pozzo C, Poston G et al; European Colorectal Metastases Treatment Group . Towards a pan‐European consensus on the treatment of patients with colorectal liver metastases. Eur J Cancer 2006; 42: 2212–2221. - PubMed
-
- Imai K, Allard MA, Castro Benitez C, Vibert E, Sa Cunha A, Cherqui D et al Long‐term outcomes of radiofrequency ablation combined with hepatectomy compared with hepatectomy alone for colorectal liver metastases. Br J Surg 2017; 104: 570–579. - PubMed
-
- Tomlinson JS, Jarnagin WR, DeMatteo RP, Fong Y, Kornprat P, Gonen M et al Actual 10‐year survival after resection of colorectal liver metastases defines cure. J Clin Oncol 2007; 25: 4575–4580. - PubMed
-
- Blazer DG III, Kishi Y, Maru DM, Kopetz S, Chun YS, Overman MJ et al Pathologic response to preoperative chemotherapy: a new outcome end point after resection of hepatic colorectal metastases. J Clin Oncol 2008; 26: 5344–5351. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
