

Gastric perforation secondary to an incarcerated paraesophageal hernia
- PMID: 31183595
- PMCID: PMC6557949
- DOI: 10.1186/s40792-019-0653-2
Gastric perforation secondary to an incarcerated paraesophageal hernia
Abstract
Background: Paraesophageal hernias are usually asymptomatic; however, they can cause serious complications such as necrosis or incarceration-induced perforation. Necrosis usually occurs in the incarcerated portion of the hernia. Here, we report the case of a patient with gastric necrosis secondary to an incarcerated paraesophageal hernia in which the necrotic lesion was outside the hernia sac.
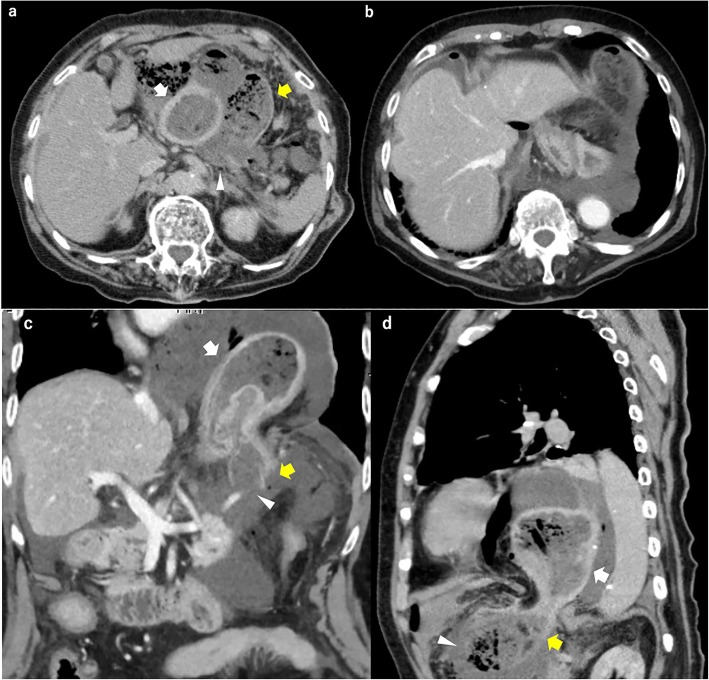
Case presentation: A 91-year-old woman presented with severe abdominal pain and vomiting. A physical examination showed hypotension and a diffusely tender and rigid abdomen. Computed tomography showed a paraesophageal hernia, massive ascites, and free air around the stomach. A laparotomy was performed to treat the upper gastrointestinal perforation. The stomach was incarcerated within the paraesophageal hernia sac. After reducing the stomach, we identified a large perforation on the posterior wall of the gastric fundus. Full-thickness necrosis involving part of the stomach necessitated total gastrectomy. She remained physiologically unstable and her condition deteriorated; she died 2 days postoperatively.
Conclusions: A hiatal hernia can be associated with an ischemic gastric perforation outside the hernia sac.
Keywords: Gastrectomy; Gastric perforation; Paraesophageal hernia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
LinkOut - more resources
Full Text Sources
