

Variation in Physicians' Electronic Health Record Documentation and Potential Patient Harm from That Variation
- PMID: 31183688
- PMCID: PMC6848521
- DOI: 10.1007/s11606-019-05025-3
Variation in Physicians' Electronic Health Record Documentation and Potential Patient Harm from That Variation
Abstract
Background: Physician-to-physician variation in electronic health record (EHR) documentation not driven by patients' clinical status could be harmful.
Objective: Measure variation in completion of common clinical documentation domains. Identify perceived causes and effects of variation and strategies to mitigate negative effects.
Design: Sequential, explanatory, mixed methods using log data from a commercial EHR vendor and semi-structured interviews with outpatient primary care practices.
Participants: Quantitative: 170,332 encounters led by 809 physicians in 237 practices. Qualitative: 40 interviewees in 10 practices.
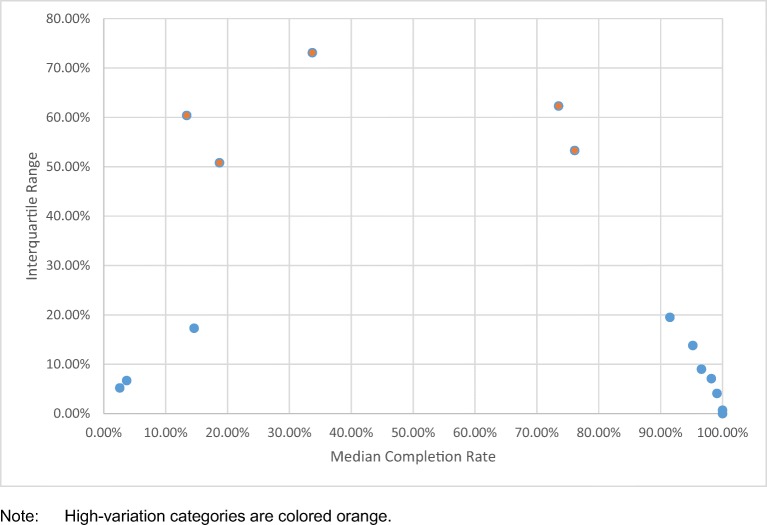
Main measures: Interquartile range (IQR) of the proportion of encounters in which a physician completed documentation, for each documentation category. Multilevel linear regression measured the proportion of variation at the physician level.
Key results: Five clinical documentation categories had substantial and statistically significant (p < 0.001) variation at the physician level after accounting for state, organization, and practice levels: (1) discussing results (IQR = 50.8%, proportion of variation explained by physician level = 78.1%); (2) assessment and diagnosis (IQR = 60.4%, physician-level variation = 76.0%); (3) problem list (IQR = 73.1%, physician-level variation = 70.1%); (4) review of systems (IQR = 62.3%, physician-level variation = 67.7%); and (5) social history (IQR = 53.3%, physician-level variation = 62.2%). Drivers of variation from interviews included user preferences and EHR designs with multiple places to record similar information. Variation was perceived to create documentation inefficiencies and risk patient harm due to missed or misinterpreted information. Mitigation strategies included targeted user training during EHR implementation and practice meetings focused on documentation standardization.
Conclusions: Physician-to-physician variation in EHR documentation impedes effective and safe use of EHRs, but there are potential strategies to mitigate negative consequences.
Keywords: EHR; documentation; mixed methods; primary care.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Forced Inefficiencies of the Electronic Health Record.J Gen Intern Med. 2019 Nov;34(11):2299-2301. doi: 10.1007/s11606-019-05281-3. J Gen Intern Med. 2019. PMID: 31452040 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
