

Altered Movement Biomechanics in Chronic Ankle Instability, Coper, and Control Groups: Energy Absorption and Distribution Implications
- PMID: 31184955
- PMCID: PMC6602392
- DOI: 10.4085/1062-6050-483-17
Altered Movement Biomechanics in Chronic Ankle Instability, Coper, and Control Groups: Energy Absorption and Distribution Implications
Erratum in
-
Erratum.J Athl Train. 2020 Jan;55(1):5. doi: 10.4085/1062-6050-483-17.E1. J Athl Train. 2020. PMID: 31935143 Free PMC article. No abstract available.
Abstract
Context: Patients with chronic ankle instability (CAI) exhibit deficits in neuromuscular control, resulting in altered movement strategies. However, no researchers have examined neuromuscular adaptations to dynamic movement strategies during multiplanar landing and cutting among patients with CAI, individuals who are ankle-sprain copers, and control participants.
Objective: To investigate lower extremity joint power, stiffness, and ground reaction force (GRF) during a jump-landing and cutting task among CAI, coper, and control groups.
Design: Cross-sectional study.
Setting: Laboratory.
Patients or other participants: A total of 22 patients with CAI (age = 22.7 ± 2.0 years, height = 174.6 ± 10.4 cm, mass = 73.4 ± 12.1 kg), 22 ankle-sprain copers (age = 22.1 ± 2.1 years, height = 173.8 ± 8.2 cm, mass = 72.6 ± 12.3 kg), and 22 healthy control participants (age = 22.5 ± 3.3 years, height = 172.4 ± 13.3 cm, mass = 72.6 ± 18.7 kg).
Intervention(s): Participants performed 5 successful trials of a jump-landing and cutting task.
Main outcome measure(s): Using motion-capture cameras and a force plate, we collected lower extremity ankle-, knee-, and hip-joint power and stiffness and GRFs during the jump-landing and cutting task. Functional analyses of variance were used to evaluate between-groups differences in these dependent variables throughout the contact phase of the task.
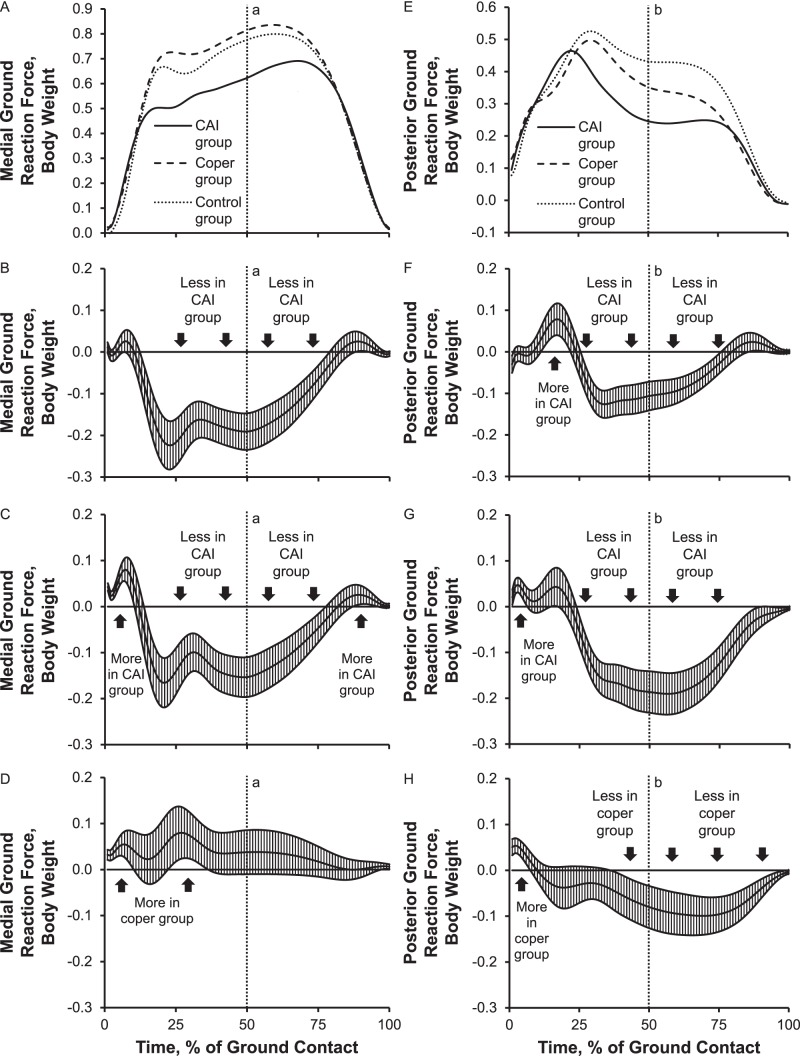
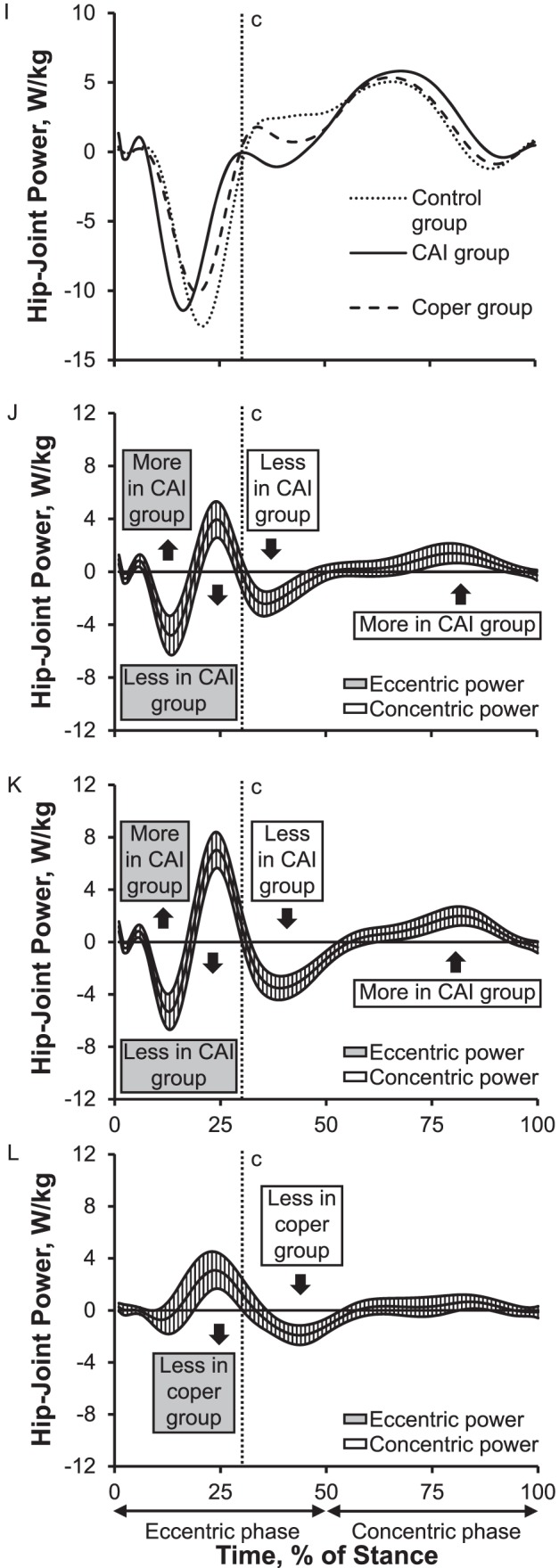
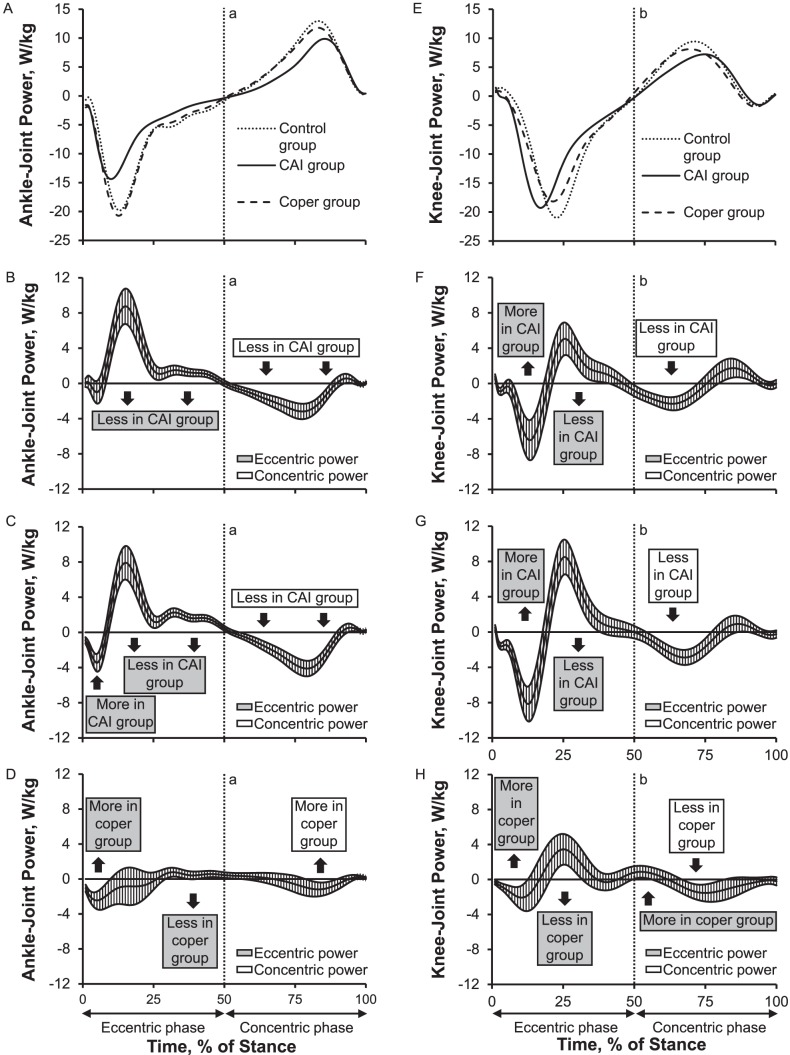
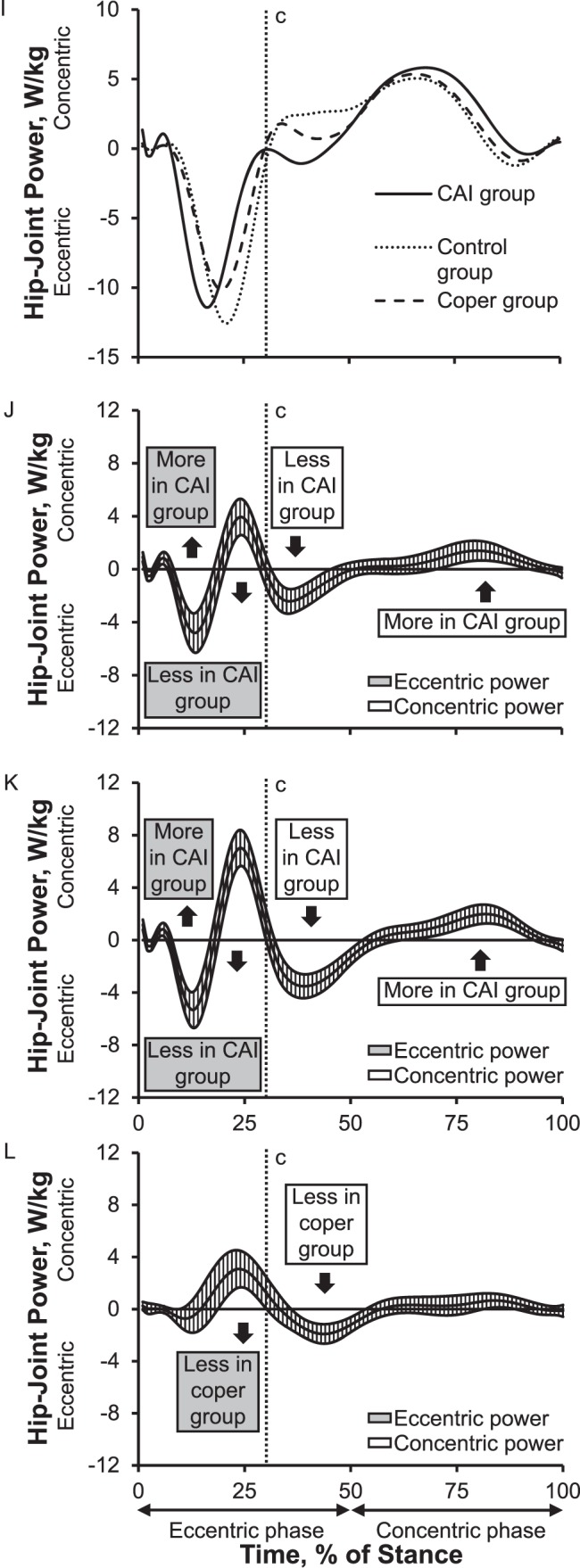
Results: Compared with the coper and control groups, the CAI group displayed (1) up to 7% of body weight more posterior and 52% of body weight more vertical GRF during initial landing followed by decreased GRF during the remaining stance and 22% of body weight less medial GRF across most of stance; (2) 8.8 W/kg less eccentric and 3.2 W/kg less concentric ankle power, 6.4 W/kg more eccentric knee and 4.8 W/kg more eccentric hip power during initial landing, and 5.0 W/kg less eccentric knee and 3.9 W/kg less eccentric hip power; and (3) less ankle- and knee-joint stiffness during the landing phase. Concentric power patterns were similar to eccentric power patterns.
Conclusions: The CAI group demonstrated altered neuromechanics, redistributing energy absorption from the distal (ankle) to the proximal (knee and hip) joints, which coincided with decreased ankle and knee stiffness during landing. Our data suggested that although the coper and control groups showed similar landing and cutting strategies, the CAI group used altered strategies to modulate impact forces during the task.
Keywords: ankle sprains; energetics; ground reaction forces; kinetics; landing mechanics.
Figures
Similar articles
-
Altered movement strategies during jump landing/cutting in patients with chronic ankle instability.Scand J Med Sci Sports. 2019 Aug;29(8):1130-1140. doi: 10.1111/sms.13445. Epub 2019 May 29. Scand J Med Sci Sports. 2019. PMID: 31050053
-
Lower Limb Joint Kinetics During a Side-Cutting Task in Participants With or Without Chronic Ankle Instability.J Athl Train. 2020 Feb;55(2):169-175. doi: 10.4085/1062-6050-334-18. Epub 2020 Jan 2. J Athl Train. 2020. PMID: 31895591 Free PMC article.
-
Single-leg drop landing movement strategies in participants with chronic ankle instability compared with lateral ankle sprain 'copers'.Knee Surg Sports Traumatol Arthrosc. 2016 Apr;24(4):1049-59. doi: 10.1007/s00167-015-3852-9. Epub 2015 Nov 14. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 26572632
-
Individuals with chronic ankle instability exhibit dynamic postural stability deficits and altered unilateral landing biomechanics: A systematic review.Phys Ther Sport. 2019 May;37:210-219. doi: 10.1016/j.ptsp.2018.06.003. Epub 2018 Jun 13. Phys Ther Sport. 2019. PMID: 29914742
-
Ankle Instability Patients Exhibit Altered Muscle Activation of Lower Extremity and Ground Reaction Force during Landing: A Systematic Review and Meta-Analysis.J Sports Sci Med. 2021 Apr 15;20(2):373-390. doi: 10.52082/jssm.2021.373. eCollection 2021 Jun. J Sports Sci Med. 2021. PMID: 34211331 Free PMC article.
Cited by
-
Compensatory Kinetics During the Side-Hop Test in Individuals With Chronic Ankle Instability.J Athl Train. 2023 Nov 1;58(11-12):920-926. doi: 10.4085/1062-6050-0592.22. J Athl Train. 2023. PMID: 37071526 Free PMC article.
-
Effects of perceptual-cognitive tasks on inter-joint coordination of soccer players and ordinary college students.Front Psychol. 2022 Oct 5;13:892118. doi: 10.3389/fpsyg.2022.892118. eCollection 2022. Front Psychol. 2022. PMID: 36275239 Free PMC article.
-
Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes.Sports (Basel). 2022 Jul 22;10(8):111. doi: 10.3390/sports10080111. Sports (Basel). 2022. PMID: 35893658 Free PMC article.
-
Test-retest, intra- and inter-rater reliability of the reactive balance test in patients with chronic ankle instability.Front Neurol. 2024 Feb 16;15:1320043. doi: 10.3389/fneur.2024.1320043. eCollection 2024. Front Neurol. 2024. PMID: 38434204 Free PMC article.
-
Construction and validation of a nomogram model for predicting different sites of ankle pain in runners with chronic ankle instability.Sci Rep. 2024 Sep 27;14(1):22337. doi: 10.1038/s41598-024-71688-6. Sci Rep. 2024. PMID: 39333581 Free PMC article.
References
-
- Roos KG, Kerr ZY, Mauntel TC, Djoko A, Dompier TP, Wikstrom EA. The epidemiology of lateral ligament complex ankle sprains in National Collegiate Athletic Association sports. Am J Sports Med. 2017;45(1):201–209. - PubMed
-
- Feger MA, Glaviano NR, Donovan L, et al. Current trends in the management of lateral ankle sprain in the United States. Clin J Sport Med. 2017;27(2):145–152. - PubMed
-
- Docherty CL, Arnold BL, Zinder SM, Granata K, Gansneder BM. Relationship between two proprioceptive measures and stiffness at the ankle. J Electromyogr Kinesiol. 2004;14(3):317–324. - PubMed
-
- Terrier R, Rose-Dulcina K, Toschi B, Forestier N. Impaired control of weight bearing ankle inversion in subjects with chronic ankle instability. Clin Biomech (Bristol, Avon) 2014;29(4):439–443. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
