

The Ankle-Joint Complex: A Kinesiologic Approach to Lateral Ankle Sprains
- PMID: 31184957
- PMCID: PMC6602390
- DOI: 10.4085/1062-6050-472-17
The Ankle-Joint Complex: A Kinesiologic Approach to Lateral Ankle Sprains
Abstract
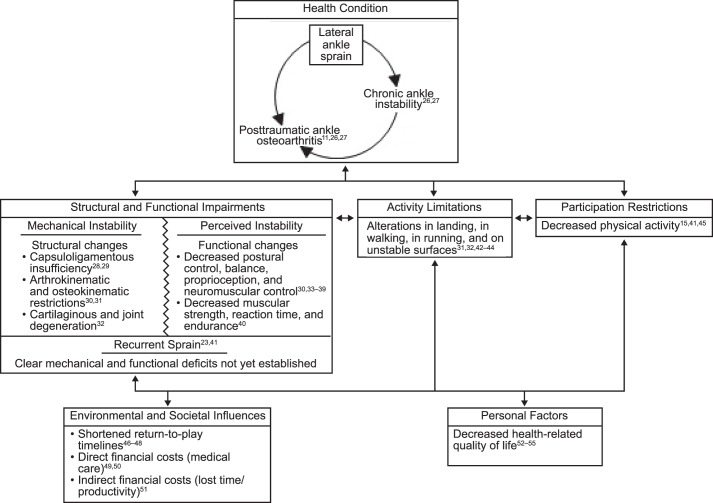
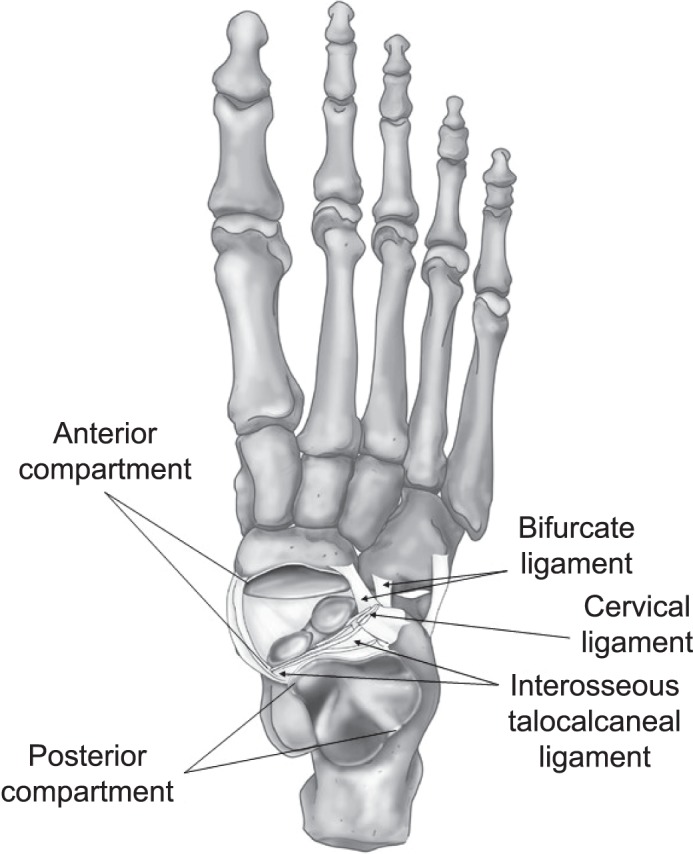
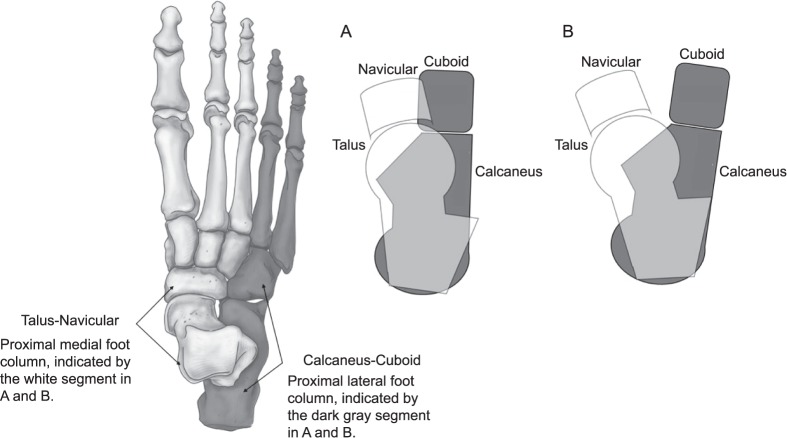
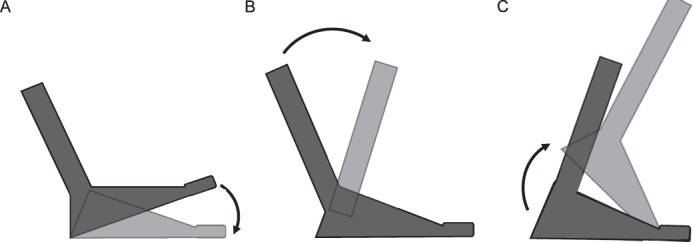
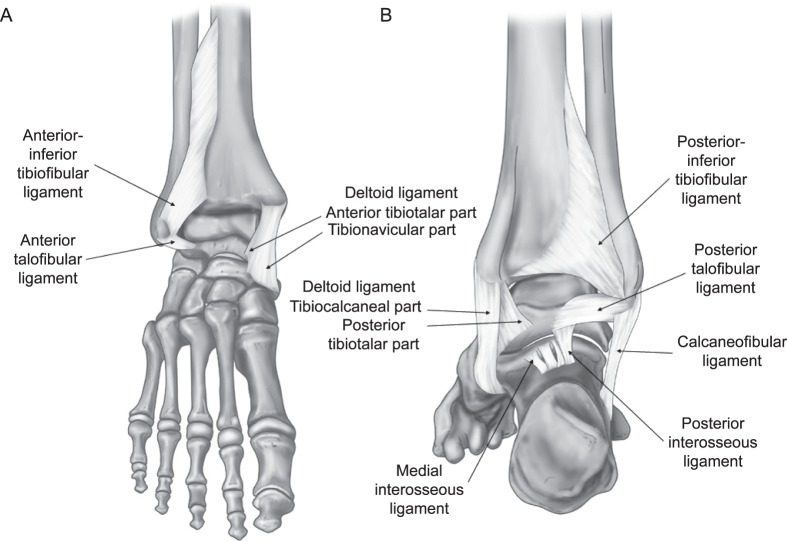
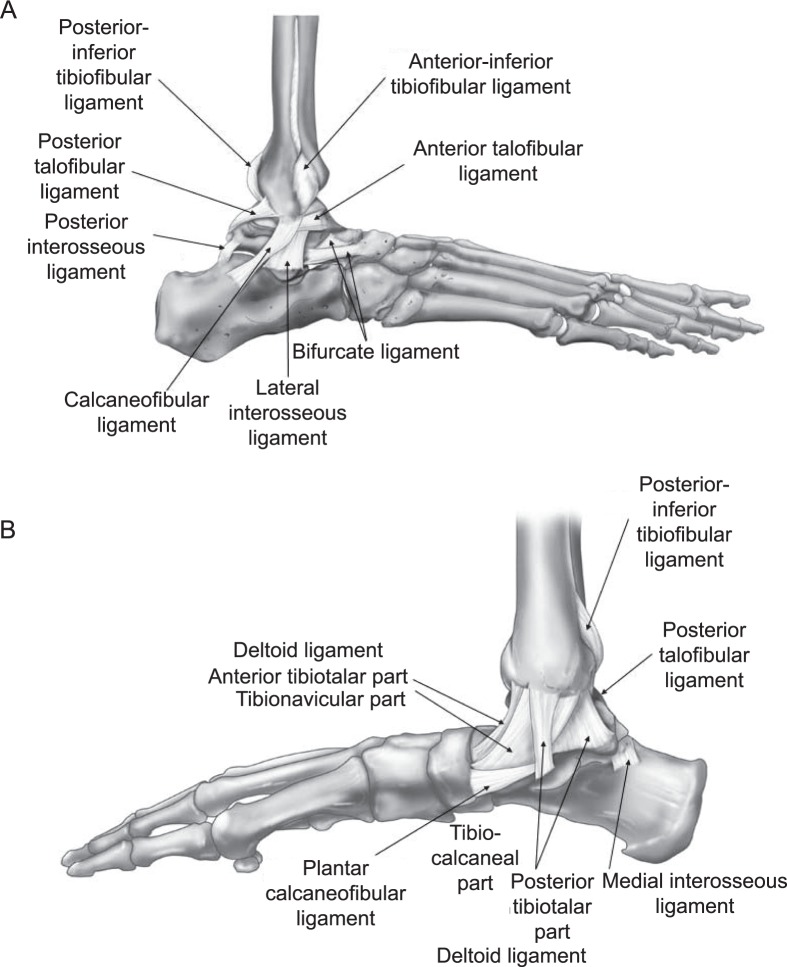
Copious research exists regarding ankle instability, yet lateral ankle sprains (LASs) persist in being among the most common recurrent musculoskeletal injuries. Key anatomical structures of the ankle include a triform articulating structure that includes the inferior tibiofibular, talocrural, and subtalar joints. Functionally, force absorption and propulsion through the ankle complex are necessary for any task that occurs in weight bearing. For optimal ankle performance and avoidance of injury, an intricate balance between stability and mobility is necessary to ensure that appropriate force transfer occurs during sports and activities of daily living. Consideration for the many structures that may be directly or indirectly involved in LASs will likely translate into advancements in clinical care. In this clinical review, we present the structure, function, and relevant pathologic states of the ankle complex to stimulate a better understanding of the prevention, evaluation, and treatment of LASs.
Keywords: anatomy; biomechanics; joint injury; lower extremity.
Figures
References
-
- Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle: operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73(2):305–312. - PubMed
-
- Fernandez WG, Yard EE, Comstock RD. Epidemiology of lower extremity injuries among U.S. high school athletes. Acad Emerg Med. 2007;14(7):641–645. - PubMed
-
- Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123–140. - PubMed
-
- de Bie RA, de Vet HC, van den Wildenberg FA, Lenssen T, Knipschild PG. The prognosis of ankle sprains. Int J Sports Med. 1997;18(4):285–289. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
