

Sleep in the United States Military
- PMID: 31185484
- PMCID: PMC6879759
- DOI: 10.1038/s41386-019-0431-7
Sleep in the United States Military
Abstract
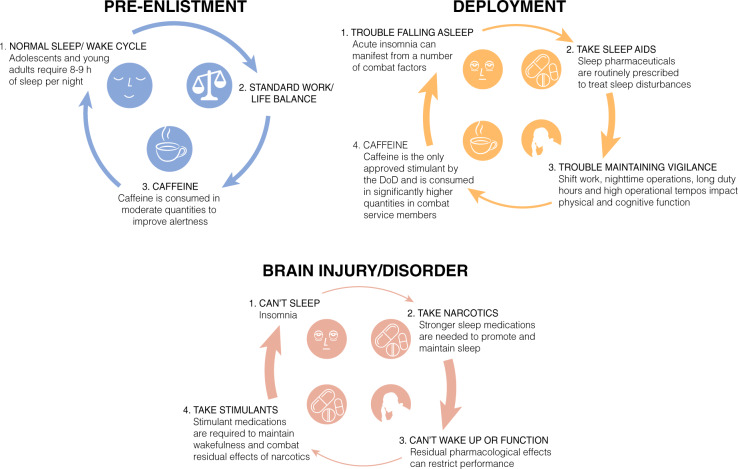
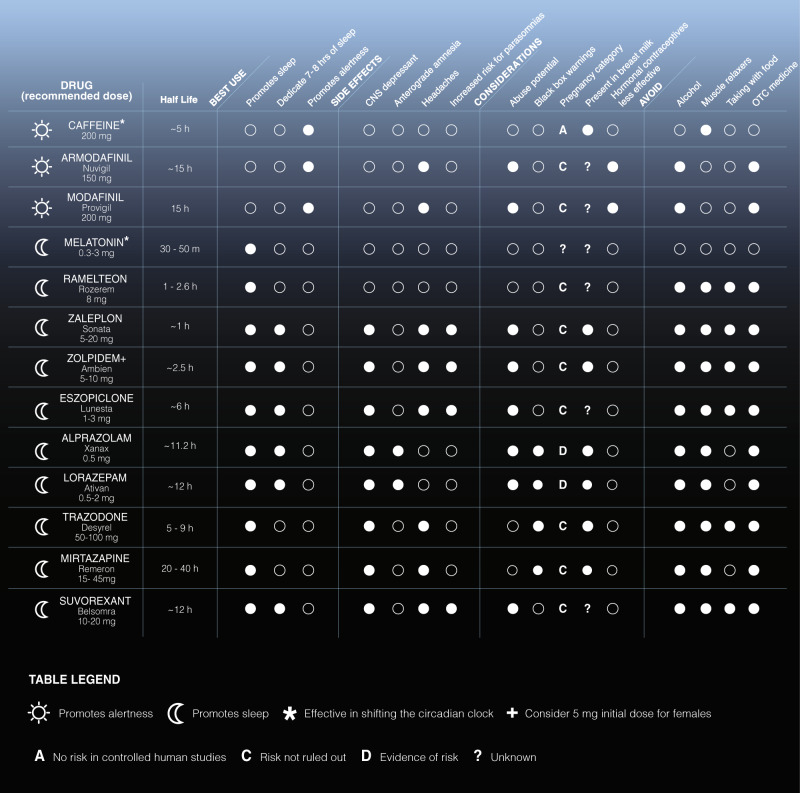
The military lifestyle often includes continuous operations whether in training or deployed environments. These stressful environments present unique challenges for service members attempting to achieve consolidated, restorative sleep. The significant mental and physical derangements caused by degraded metabolic, cardiovascular, skeletomuscular, and cognitive health often result from insufficient sleep and/or circadian misalignment. Insufficient sleep and resulting fatigue compromises personal safety, mission success, and even national security. In the long-term, chronic insufficient sleep and circadian rhythm disorders have been associated with other sleep disorders (e.g., insomnia, obstructive sleep apnea, and parasomnias). Other physiologic and psychologic diagnoses such as post-traumatic stress disorder, cardiovascular disease, and dementia have also been associated with chronic, insufficient sleep. Increased co-morbidity and mortality are compounded by traumatic brain injury resulting from blunt trauma, blast exposure, and highly physically demanding tasks under load. We present the current state of science in human and animal models specific to service members during- and post-military career. We focus on mission requirements of night shift work, sustained operations, and rapid re-entrainment to time zones. We then propose targeted pharmacological and non-pharmacological countermeasures to optimize performance that are mission- and symptom-specific. We recognize a critical gap in research involving service members, but provide tailored interventions for military health care providers based on the large body of research in health care and public service workers.
Figures
References
-
- Capener DC, Brock MS, Hansen SL, Matsangas P, Mysliwiec V. An initial report of sleep disorders in women in the U.S. Military. Mil Med. 2018;183:e266–e271. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
