

Long-term effects on PTH and mineral metabolism of 1.25 versus 1.75 mmol/L dialysate calcium in peritoneal dialysis patients: a meta-analysis
- PMID: 31185931
- PMCID: PMC6558799
- DOI: 10.1186/s12882-019-1388-9
Long-term effects on PTH and mineral metabolism of 1.25 versus 1.75 mmol/L dialysate calcium in peritoneal dialysis patients: a meta-analysis
Abstract
Background: This study aimed to compare 1.25 and 1.75 mmol/L dialysate calcium for their effects on parathyroid hormone (PTH) and mineral metabolism in peritoneal dialysis (PD).
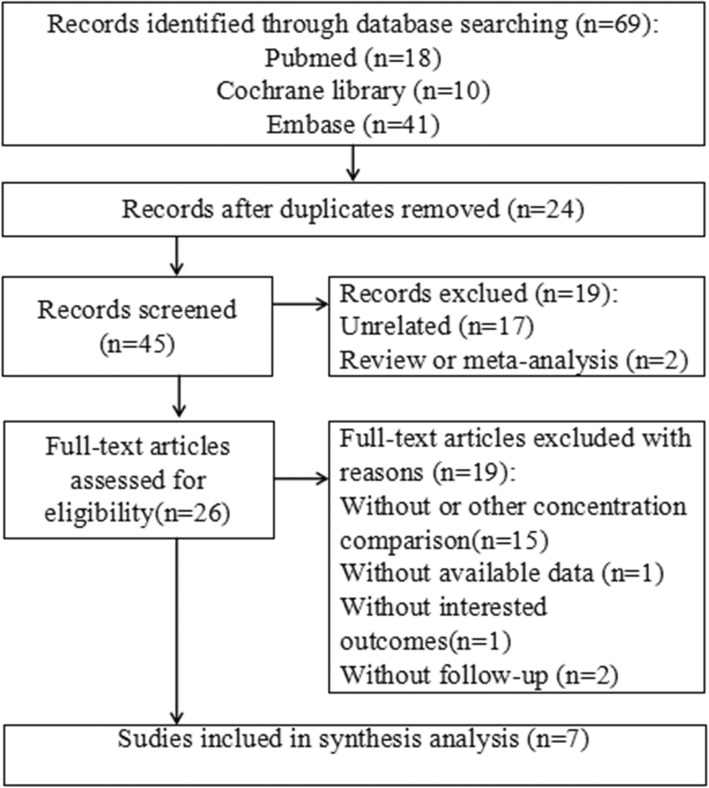
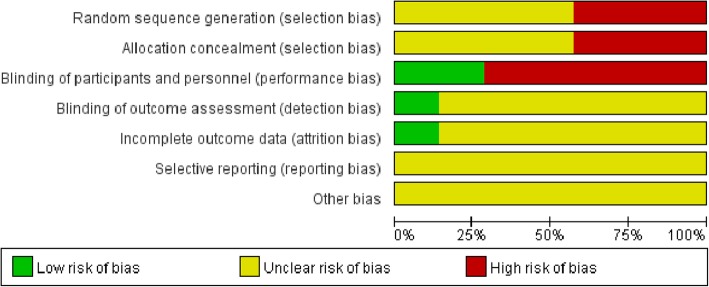
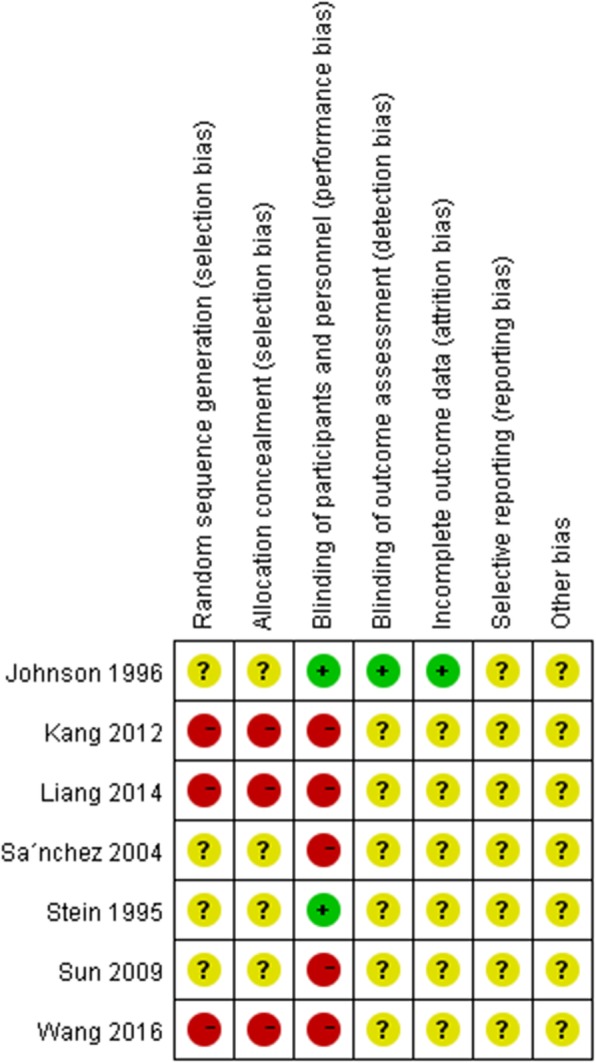
Methods: The PubMed, Cochrane Library, and EmBase databases were searched from inception to October 2016. Methodological quality assessment of the included studies was performed using the risk of bias tool of the Review Manager software. The meta-analysis was carried out with the Stata12.0 software. Subgroup analysis was performed by study design [randomized controlled trial (RCT) and non-RCT]. Odds ratios or standardized mean differences were used to assess the outcome measures, including intact parathyroid hormone (i-PTH) levels, serum total calcium amounts, ionized calcium levels, phosphate concentrations, and peritonitis episodes.
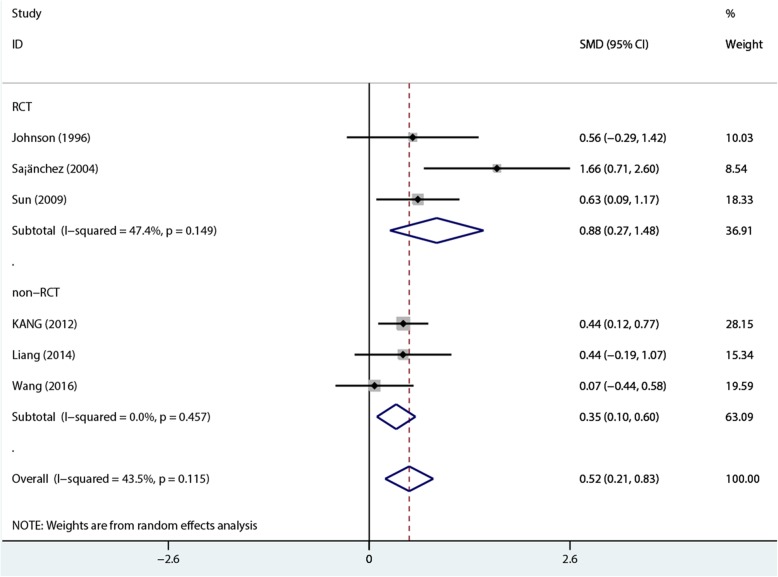
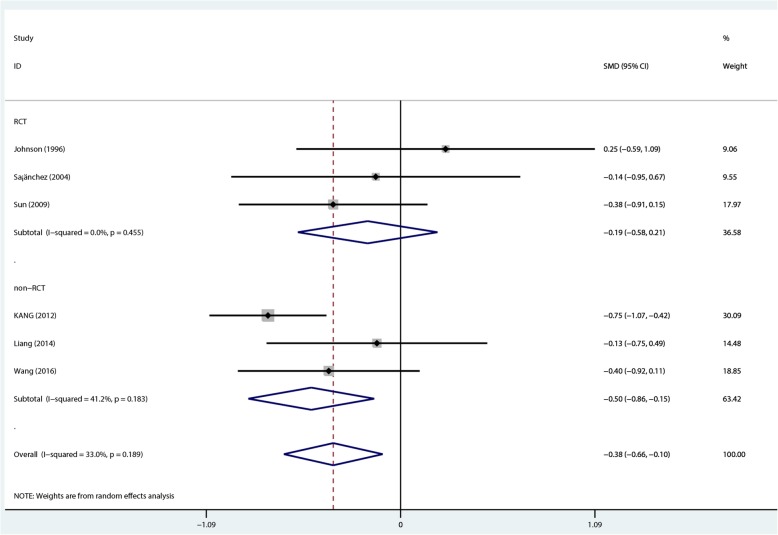
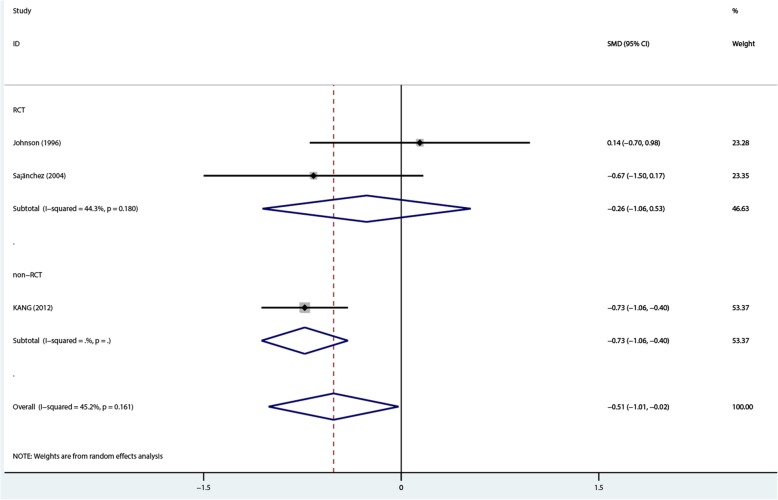
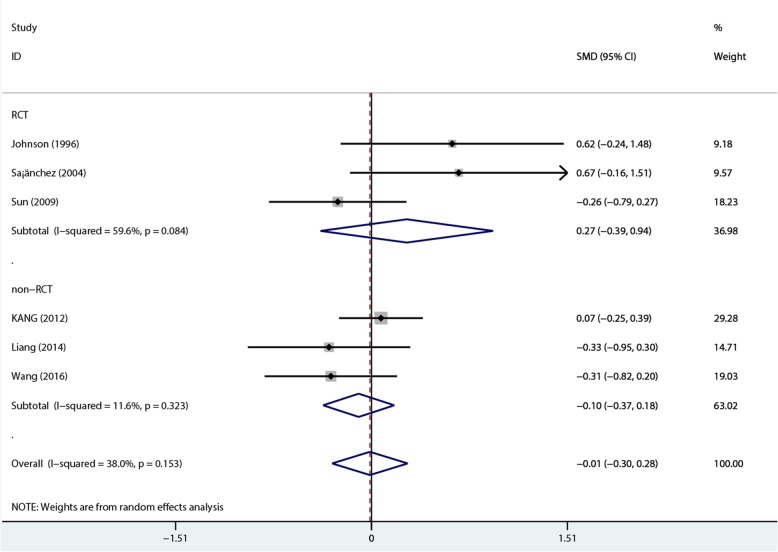
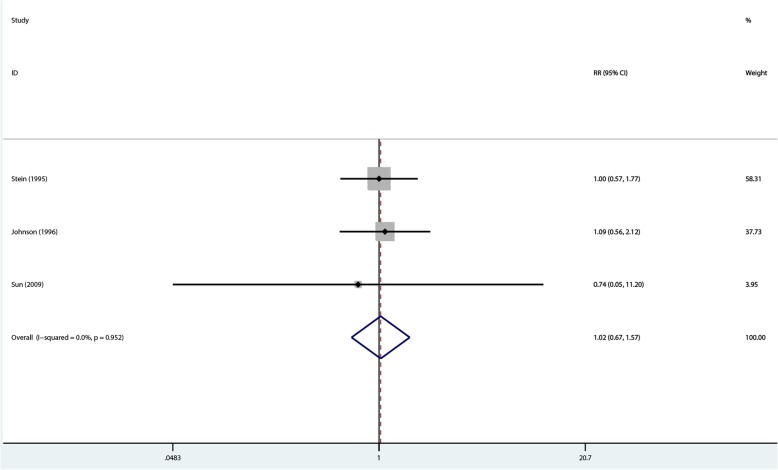
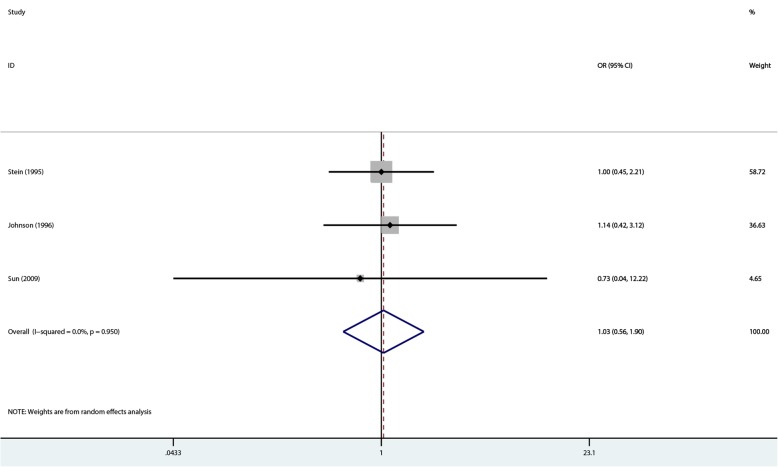
Results: Seven studies were enrolled in the synthesized analysis, including 4 RCTs and 3 non-RCTs. All studies compared 1.25 mmol/L and 1.75 mmol/L dialysate calcium for PD. Pooled analysis revealed that 1.75 mmol/L dialysate calcium significantly reduced i-PTH levels compared with the 1.25 mmol/L dose in PD patients. However, 1.25 mmol/L dialysate calcium was superior to the 1.75 mmol/L dose in decreasing the levels of serum total calcium and ionized calcium in PD patients. No significant differences in phosphate amounts and peritonitis episodes were observed between the two groups.
Conclusion: These findings indicated that 1.75 mmol/L dialysate calcium is more appropriate for PD patients with secondary hyperparathyroidism. Meanwhile, 1.25 mmol/L dialysate calcium is more favorable to PD patients with secondary hypercalcemia. However, further well-designed and high-quality studies are required to validate these findings.
Keywords: Dialysate calcium; Intact parathyroid hormone; Meta-analysis; Peritoneal dialysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Long-term dialysis with low-calcium solution (1.0 mmol/L) in CAPD: effects on bone mineral metabolism. Collaborators of the Multicenter Study Group.Perit Dial Int. 1996 May-Jun;16(3):260-8. Perit Dial Int. 1996. PMID: 8761540 Clinical Trial.
-
High-normal calcium (1.35 mmol/l) dialysate in patients on CAPD: efficient and safe long-term control of plasma calcium, phosphate, and parathyroid hormone.Nephrol Dial Transplant. 1996 Aug;11(8):1586-91. Nephrol Dial Transplant. 1996. PMID: 8856216
-
Low dialysate calcium in continuous ambulatory peritoneal dialysis: a randomized controlled multicenter trial. The Peritoneal Dialysis Multicenter Study Group.Am J Kidney Dis. 1995 Mar;25(3):452-60. doi: 10.1016/0272-6386(95)90108-6. Am J Kidney Dis. 1995. PMID: 7872324 Clinical Trial.
-
Icodextrin Versus Glucose Solutions for the Once-Daily Long Dwell in Peritoneal Dialysis: An Enriched Systematic Review and Meta-analysis of Randomized Controlled Trials.Am J Kidney Dis. 2020 Jun;75(6):830-846. doi: 10.1053/j.ajkd.2019.10.004. Epub 2020 Feb 4. Am J Kidney Dis. 2020. PMID: 32033860
-
Calcium concentration in the CAPD dialysate: what is optimal and is there a need to individualize?Perit Dial Int. 1997 Nov-Dec;17(6):554-9. Perit Dial Int. 1997. PMID: 9655154 Review.
Cited by
-
Influence of low free thyroxine on progression of chronic kidney disease.BMC Nephrol. 2020 Jan 30;21(1):36. doi: 10.1186/s12882-019-1677-3. BMC Nephrol. 2020. PMID: 32000713 Free PMC article.
-
Bone Mineral Parameters in Peritoneal Dialysis Patients after Lowering Calcium Concentration in Dialysis Fluids: A Case Series in Patients Using Icodextrin.Case Rep Nephrol Dial. 2023 Nov 8;13(1):184-190. doi: 10.1159/000534476. eCollection 2023 Jan-Dec. Case Rep Nephrol Dial. 2023. PMID: 37946857 Free PMC article.
-
The Role of Daily Dialysate Calcium Exposure in Phosphaturic Hormones in Dialysis Patients.Life (Basel). 2024 Jul 31;14(8):964. doi: 10.3390/life14080964. Life (Basel). 2024. PMID: 39202706 Free PMC article.
-
A feasibility study of avoiding positive calcium balance and parathyroid hormone increase in patients on peritoneal dialysis.Bone Rep. 2022 Sep 29;17:101625. doi: 10.1016/j.bonr.2022.101625. eCollection 2022 Dec. Bone Rep. 2022. PMID: 36217349 Free PMC article.
-
Factors affecting the relationship between ionized and corrected calcium levels in peritoneal dialysis patients: a retrospective cross-sectional study.BMC Nephrol. 2020 Aug 26;21(1):370. doi: 10.1186/s12882-020-02033-y. BMC Nephrol. 2020. PMID: 32847525 Free PMC article.
References
-
- Borzych D, Rees L, Ha IS, Chua A, Valles PG, Lipka M, Zambrano P, Ahlenstiel T, Bakkaloglu SA, Spizzirri AP, Lopez L, Ozaltin F, Printza N, Hari P, Klaus G, Bak M, Vogel A, Ariceta G, Yap HK, Warady BA, Schaefer F. The bone and mineral disorder of children undergoing chronic peritoneal dialysis. Kidney Int. 2010;78:1295–1304. doi: 10.1038/ki.2010.316. - DOI - PubMed
-
- Young EW, Albert JM, Satayathum S, Goodkin DA, Pisoni RL, Akiba T, Akizawa T, Kurokawa K, Bommer J, Piera L, Port FK. Predictors and consequences of altered mineral metabolism: the Dialysis outcomes and practice patterns study. Kidney Int. 2005;67:1179–1187. doi: 10.1111/j.1523-1755.2005.00185.x. - DOI - PubMed
-
- Mesquita M, Wittersheim E, Demulder A, Dratwa M, Bergmann P. Bone cytokines and renal osteodystrophy in peritoneal dialysis patients. Adv Perit Dial. 2005;21:181–184. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
