

Triglyceride deposit cardiomyovasculopathy: a rare cardiovascular disorder
- PMID: 31186072
- PMCID: PMC6560904
- DOI: 10.1186/s13023-019-1087-4
Triglyceride deposit cardiomyovasculopathy: a rare cardiovascular disorder
Abstract
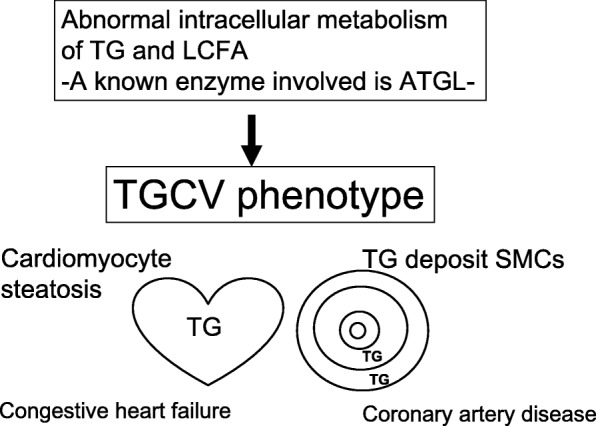
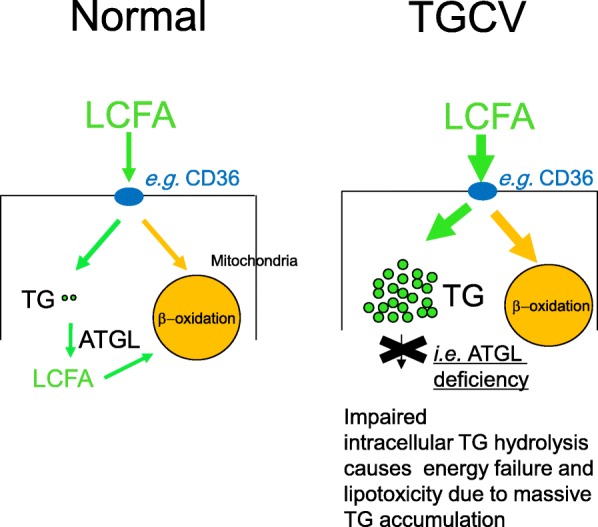
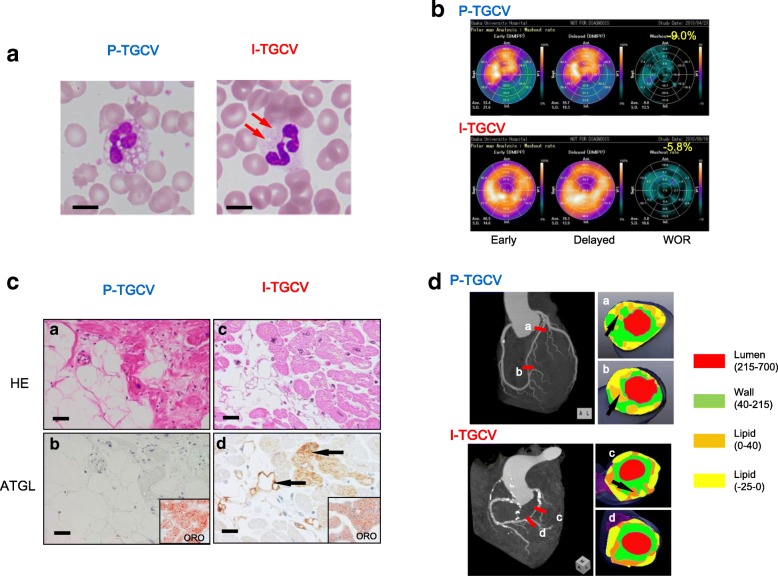
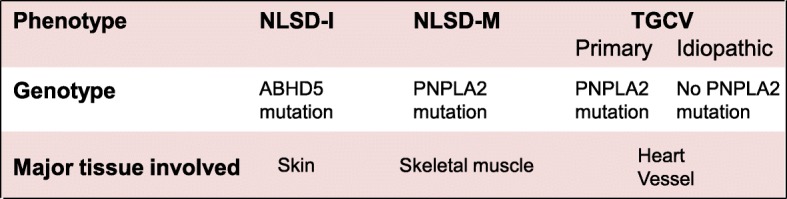
Triglyceride deposit cardiomyovasculopathy (TGCV) is a phenotype primarily reported in patients carrying genetic mutations in PNPLA2 encoding adipose triglyceride lipase (ATGL) which releases long chain fatty acid (LCFA) as a major energy source by the intracellular TG hydrolysis. These patients suffered from intractable heart failure requiring cardiac transplantation. Moreover, we identified TGCV patients without PNPLA2 mutations based on pathological and clinical studies. We provided the diagnostic criteria, in which TGCV with and without PNPLA2 mutations were designated as primary TGCV (P-TGCV) and idiopathic TGCV (I-TGCV), respectively. We hereby report clinical profiles of TGCV patients. Between 2014 and 2018, 7 P-TGCV and 18 I-TGCV Japanese patients have been registered in the International Registry. Patients with I-TGCV, of which etiologies and causes are not known yet, suffered from adult-onset severe heart disease, including heart failure and coronary artery disease, associated with a marked reduction in ATGL activity and myocardial washout rate of LCFA tracer, as similar to those with P-TGCV. The present first registry-based study showed that TGCV is an intractable, at least at the moment, and heterogeneous cardiovascular disorder.
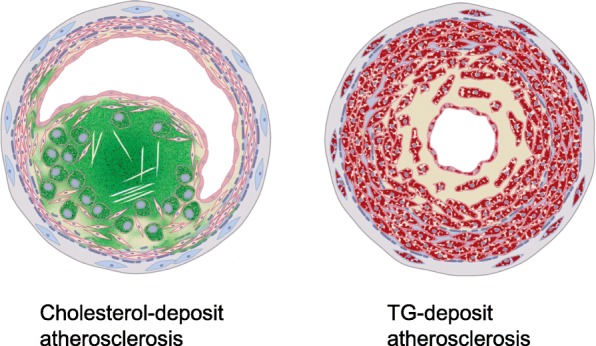
Keywords: Adipose triglyceride lipase; Atherosclerosis; Rare disease; Triglyceride metabolism; Triglyceride-deposit cardiomyovasculopathy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Genetic mutations in adipose triglyceride lipase and myocardial up-regulation of peroxisome proliferated activated receptor-γ in patients with triglyceride deposit cardiomyovasculopathy.Biochem Biophys Res Commun. 2014 Jan 10;443(2):574-9. doi: 10.1016/j.bbrc.2013.12.003. Epub 2013 Dec 8. Biochem Biophys Res Commun. 2014. PMID: 24332944
-
Newly developed selective immunoinactivation assay revealed reduction in adipose triglyceride lipase activity in peripheral leucocytes from patients with idiopathic triglyceride deposit cardiomyovasculopathy.Biochem Biophys Res Commun. 2018 Jan 1;495(1):646-651. doi: 10.1016/j.bbrc.2017.11.070. Epub 2017 Nov 13. Biochem Biophys Res Commun. 2018. PMID: 29146190
-
Tricaprin Rescues Myocardial Abnormality in a Mouse Model of Triglyceride Deposit Cardiomyovasculopathy.J Oleo Sci. 2018 Aug 1;67(8):983-989. doi: 10.5650/jos.ess18037. Epub 2018 Jul 17. J Oleo Sci. 2018. PMID: 30012901
-
The Diagnostic Criteria 2020 for Triglyceride Deposit Cardiomyovasculopathy.Ann Nucl Cardiol. 2020;6(1):99-104. doi: 10.17996/anc.20-00131. Epub 2020 Aug 31. Ann Nucl Cardiol. 2020. PMID: 37123492 Free PMC article. Review.
-
A novel mutation in PNPLA2 causes neutral lipid storage disease with myopathy and triglyceride deposit cardiomyovasculopathy: a case report and literature review.Neuromuscul Disord. 2014 Jul;24(7):634-41. doi: 10.1016/j.nmd.2014.04.001. Epub 2014 Apr 21. Neuromuscul Disord. 2014. PMID: 24836204 Review.
Cited by
-
Detection of Jordans' anomaly using compact-type automated hematology analyzer.Int J Hematol. 2019 Aug;110(2):129-130. doi: 10.1007/s12185-019-02689-9. Epub 2019 Jun 10. Int J Hematol. 2019. PMID: 31183815 No abstract available.
-
Correlation Perspectives for the Diagnosis of Idiopathic Triglyceride Deposit Cardiomyovasculopathy.Ann Nucl Cardiol. 2020;6(1):33-38. doi: 10.17996/anc.20-00128. Epub 2020 Aug 31. Ann Nucl Cardiol. 2020. PMID: 37123494 Free PMC article.
-
Triglyceride Deposit Cardiomyovasculopathy with Massive Myocardial Triglyceride which Was Proven Using Proton-magnetic Resonance Spectroscopy.Intern Med. 2021 Apr 15;60(8):1217-1220. doi: 10.2169/internalmedicine.6126-20. Epub 2020 Nov 9. Intern Med. 2021. PMID: 33162485 Free PMC article.
-
Chronic kidney disease is a major risk factor for mortality in triglyceride deposit cardiomyovasculopathy patients.Clin Exp Nephrol. 2025 Jun;29(6):866-871. doi: 10.1007/s10157-024-02618-z. Epub 2025 Jan 15. Clin Exp Nephrol. 2025. PMID: 39809936 Free PMC article.
-
A prospective randomized study comparing effects of empagliflozin to sitagliptin on cardiac fat accumulation, cardiac function, and cardiac metabolism in patients with early-stage type 2 diabetes: the ASSET study.Cardiovasc Diabetol. 2021 Feb 2;20(1):32. doi: 10.1186/s12933-021-01228-3. Cardiovasc Diabetol. 2021. PMID: 33530982 Free PMC article. Clinical Trial.
References
-
- Zimmermann R, Strauss JG, Haemmerle G, Schoiswhol G, Birner-Gruenberger R, Riedere M, Lass A, Neuberger G, Eisenhaber F, Hermetter A, Zechner R. Fat mobilization in adipose tissue is promoted by adipose triglyceride lipase. Science. 2004;306(5700):1383–1386. doi: 10.1126/science.1100747. - DOI - PubMed
-
- Haemmerle G, Lass A, Zimmermann G, Gorkiewicz G, Meyer C, Rozman J, Heldmaier G, Maier R, Theussl C, Eder S, Kratky D, Wagner EF, Klingenspor M, Hoefler G, Zechner R. Defective lipolysis and altered energy metabolism in mice lacking adipose triglyceride lipase. Science. 2006;312(5774):734–737. doi: 10.1126/science.1123965. - DOI - PubMed
-
- Schweiger M, Schoiswohl G, Lass G, Radner FP, Haemmerle G, Malli R, Graier W, Cornaciu I, Oberer M, Salvayre R, Fischer J, Zechner R, Zimmerman G. The C-terminal region of human adipose triglyceride lipase affects enzyme activity and lipid droplet binding. J Biol Chem. 2008;283(25):17211–17220. doi: 10.1074/jbc.M710566200. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
