

Clinical Outcome of Ampullary Carcinoma: Single Cancer Center Experience
- PMID: 31186632
- PMCID: PMC6521487
- DOI: 10.1155/2019/3293509
Clinical Outcome of Ampullary Carcinoma: Single Cancer Center Experience
Abstract
Introduction: Ampullary cancers represent a subset of periampullary cancers, comprising only 0.2% all gastrointestinal cancers. Localized disease is primarily managed by a surgical intervention, called pancreaticoduodenectomy (PD), followed in many cases by the administration of adjuvant chemotherapy (CT) or chemoradiation therapy (CRT). However, there are no clear evidence-based guidelines to aid in selecting both the modality and regimen of adjuvant therapy for resected Ampullary carcinoma.
Methods: We retrospectively analyzed 54 patients at KU Cancer Center, who had undergone endoscopic resection or pancreaticoduodenectomy (PD) for Ampullary cancer from June 2006 to July 2016. We obtained patients' baseline characteristics, clinical presentation, pathology, treatment modality, recurrence pattern, and survival outcomes. The time-to-events data were compared using Kaplan-Meier methods. A univariate and multivariate Cox proportional hazards regression was performed to evaluate factors associated with overall survival (OS) and generate hazard ratios (HR).
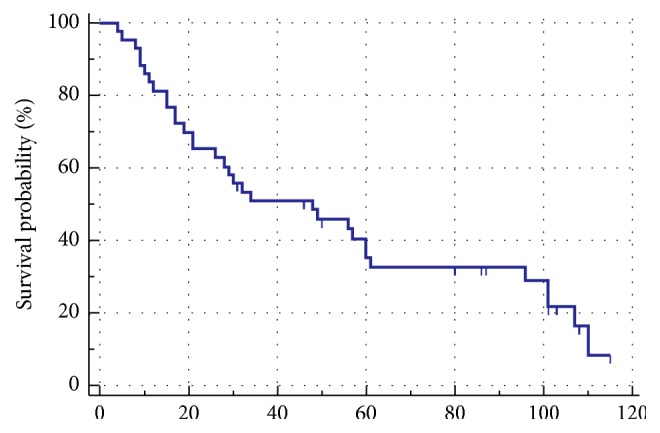
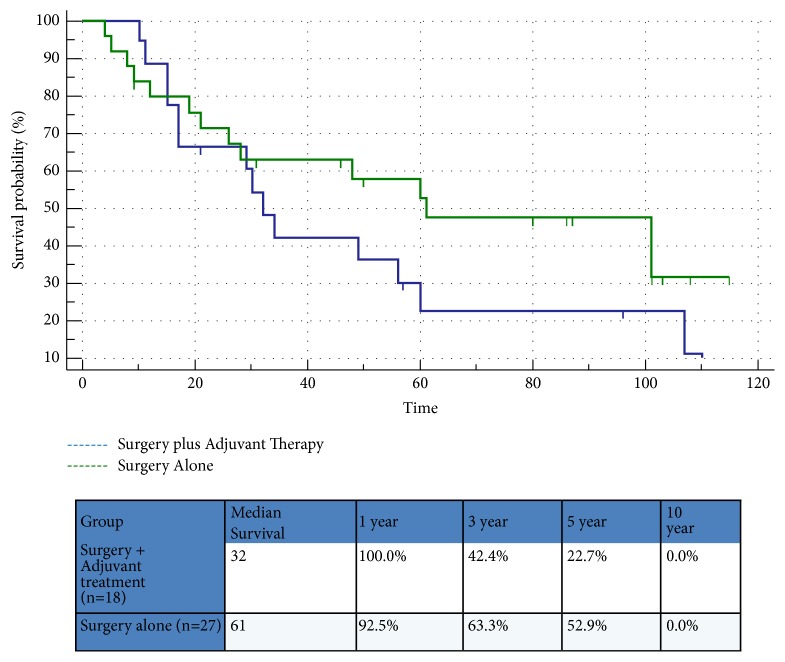
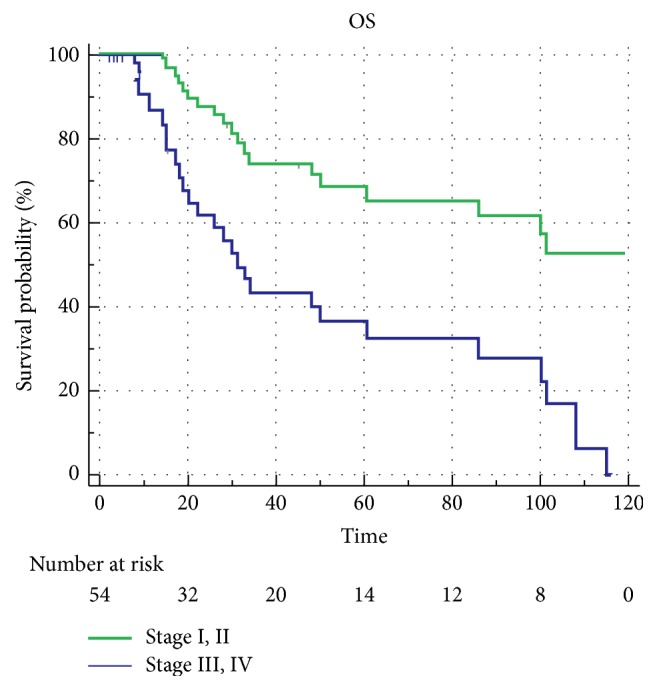
Results: The mean age of the 54 patients was 68 (37-90). 38 (70%) were males and 16 (30%) were females. Most of the patients were Caucasian (76%). Approximately half of all patients had a history of smoking, 20% had alcohol abuse, and 13% had pancreatitis. Among the 54 patients with localized cancers, 9 (16%) were treated definitively with nonoperative therapies, usually due to a prohibitive comorbidity profile, performance status, or unresectable tumor. 45 out of 54 patients (83%) underwent surgery. Of the 45 patients who underwent surgery, 18 patients (40% of the study cohort) received adjuvant therapy due to concerns for advanced disease as determined by the treating physician. 13 patients (24%) received adjuvant CT and 5 patients (9.2%) received CRT. The remaining 27 patients (50%) underwent surgery alone. The median OS for the entire study cohort was 30 months. When compared to surgery alone, adjuvant therapy with either CT or CRT had no statistically significant difference in terms of progression-free survival (p=0.56) or overall survival (p=0.80). In univariate Cox proportional hazards regression analysis, high-risk features like peripancreatic extension (16%) and perineural invasion (26%) were found to be associated with poor OS. Lymph node metastasis (29%) did not significantly affect OS (HR 1.42, 95% CI [0.73-1.86]; p=0.84). Lymphovascular invasion (29%) was not associated with poor OS (HR 1.22, 95% CI [0.52, 2.96]; p=0.76). In multivariate Cox regression analysis, only age group>70 years was significantly associated with OS , while other factors, including the receipt of adjuvant therapy, lymph nodes, positive margin, and lymphovascular, perineural, and peripancreatic involvement, were not significantly associated with OS. These results are likely due to small sample size.
Conclusions: Despite numerous advances in both cancer care and research, efforts in rare malignancies such as Ampullary cancer remain very challenging with a clear lack of an evidence-based standard of care treatment paradigm. Although adding adjuvant therapies such as chemotherapy or chemoradiotherapy is likely to improve survival in high-risk disease, there is no standardized regimen for the treatment of Ampullary cancer. More research is required to elucidate whether statistically and clinically relevant differences exist that may warrant a change in the current adjuvant treatment strategies.
Figures
References
-
- Kimura W., Ohtsubo K. Incidence, sites of origin, and immunohistochemical and histochemical characteristics of atypical epithelium and minute carcinoma of the papilla of vater. Cancer. 1988;61(7):1394–1402. doi: 10.1002/1097-0142(19880401)61:7<1394::AID-CNCR2820610720>3.0.CO;2-M. doi: 10.1002/1097-0142(19880401)61:7<1394::AID-CNCR2820610720>3.0.CO;2-M. - DOI - PubMed
-
- Herman J. M., Pawlik T. M., Merchant N. B., et al. Ampulla of vater. In: Amin M. B., editor. AJCC Cancer Staging Manual. 8th. Chicago, USA: AJCC; 2017. p. p. 327.
LinkOut - more resources
Full Text Sources
Research Materials
