

Prehabilitation before major intra-abdominal cancer surgery: A systematic review of randomised controlled trials
- PMID: 31188152
- PMCID: PMC6855314
- DOI: 10.1097/EJA.0000000000001030
Prehabilitation before major intra-abdominal cancer surgery: A systematic review of randomised controlled trials
Abstract
Background: Although prehabilitation programmes for patients undergoing major intra-abdominal cancer surgery have been shown to improve pre-operative physical fitness, the conclusions regarding any postoperative benefits are inconsistent.
Objectives: The aim of this study was to evaluate the content of and the outcome measures used in studies of prehabilitation programmes for these patients. It was hypothesised that the content of prehabilitation programmes is often therapeutically invalid, and that the postoperative outcomes assessed are inadequate to evaluate the impact of complications.
Design: A systematic review of randomised controlled trials.
Data sources: Studies published between January 2009 and January 2019 were retrieved from PubMed, Embase and PEDro.
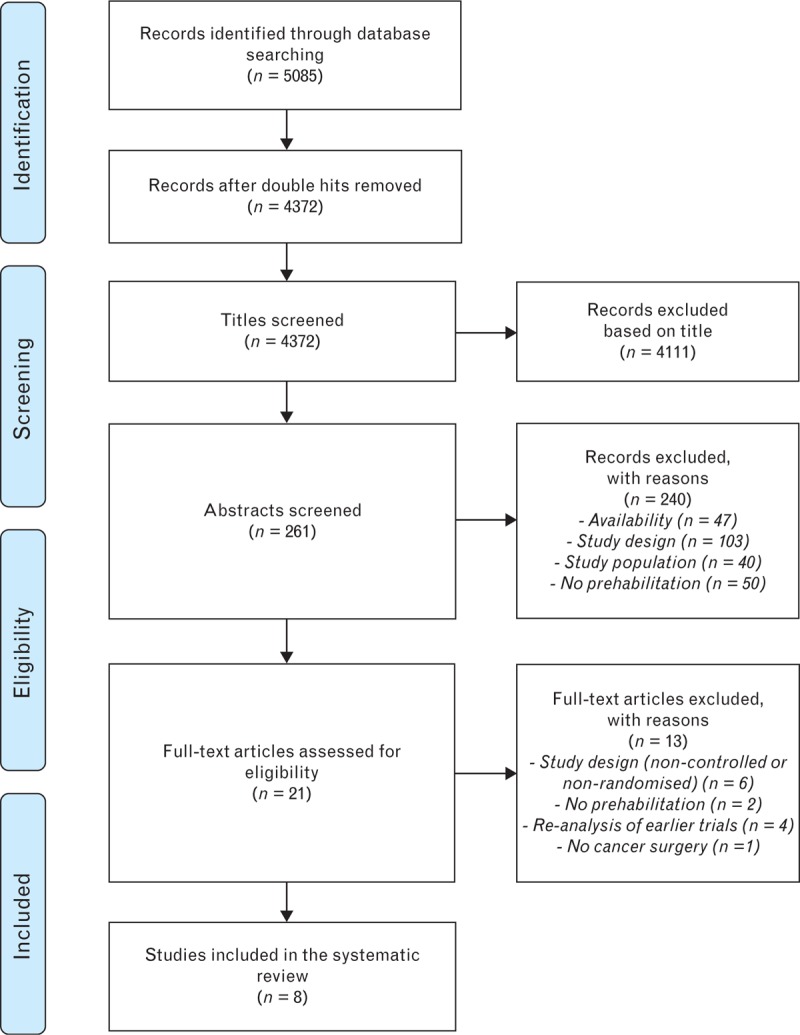
Eligibility criteria: Studies were included when they investigated the effects of prehabilitation in patients undergoing intra-abdominal surgery for cancer, reported pre-operative and/or postoperative outcome measures and were conducted as a randomised controlled trial. Studies for which the full text was not available were excluded, as were studies of patients undergoing nonabdominal cancer surgery.
Results: Eight studies (565 patients) were included. Therapeutic validity was low in five studies. Most studies included low-risk surgical patients and considerable variation was observed between prehabilitation programmes in terms of supervision, training context, frequency, intensity, duration and training type. Objective monitoring of training progression was typically not performed, and most trials did not include nutritional or psychological support. Postoperative complications were reported in seven studies, but no study reported the impact of postoperative complications, nor on long-term postoperative outcomes.
Conclusion: The content of prehabilitation programmes was heterogeneous. Studies with a high therapeutic validity found unequivocal evidence that prehabilitation had beneficial effects on postoperative outcomes. Future research should focus on adequate selection and inclusion of high-risk surgical patients and provide personalised and probably multimodal (partly) supervised prehabilitation, with objective monitoring of progress. Measuring the incidence and impact of postoperative complications may contribute to demonstrating the clinical value of prehabilitation.
Figures
References
-
- West M, Parry M, Lythgoe D, et al. Cardiopulmonary exercise testing for the prediction of morbidity risk after rectal cancer surgery. Br J Surg 2014; 101:1166–1172. - PubMed
-
- McDermott F, Heeney A, Kelly M, et al. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg 2015; 102:462–479. - PubMed
-
- Van Leersum N, Snijders H, Henneman D, et al. The Dutch surgical colorectal audit. Eur J Surg Oncol 2013; 39:1063–1070. - PubMed
-
- Wilson R, Davies S, Yates D, et al. Impaired functional capacity is associated with all-cause mortality after major elective intra-abdominal surgery. Br J Anaesth 2010; 105:297–303. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
