

Antibodies Predict Pegaspargase Allergic Reactions and Failure of Rechallenge
- PMID: 31188727
- PMCID: PMC6804844
- DOI: 10.1200/JCO.18.02439
Antibodies Predict Pegaspargase Allergic Reactions and Failure of Rechallenge
Abstract
Purpose: Pegaspargase (PEG-ASP) has largely replaced native Escherichia coli asparaginase (L-ASP) in the treatment of acute lymphoblastic leukemia because of its longer half-life and lower immunogenicity. Risk factors for allergic reactions to PEG-ASP remain unclear. Here, we identify risk factors for reactions in a front-line acute lymphoblastic leukemia trial and assess the usefulness of serum antibodies for diagnosing allergy and predicting rechallenge outcome.
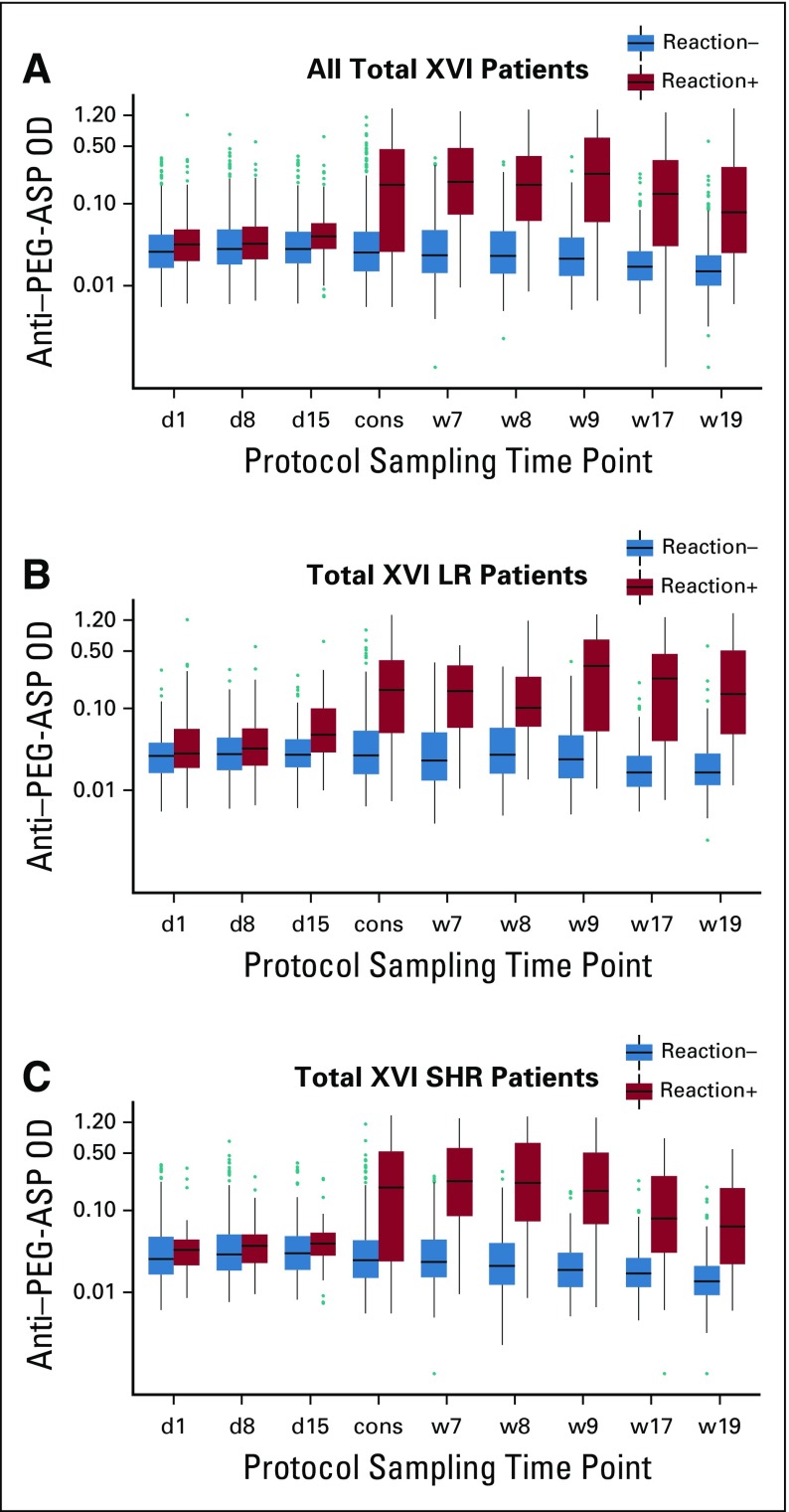
Patients and methods: PEG-ASP was administered to 598 patients in St Jude's Total XVI study. Results were compared with Total XV study (ClinicalTrials.gov identifiers: NCT00549848 and NCT00137111), which used native L-ASP. Serum samples (n = 5,369) were analyzed for anti-PEG-ASP immunoglobulin G by enzyme-linked immunosorbent assay. Positive samples were tested for anti-polyethylene glycol (PEG) and anti-L-ASP. We analyzed potential risk factors for reactions and associations between antibodies and reactions, rechallenge outcomes, and PEG-ASP pharmacokinetics.
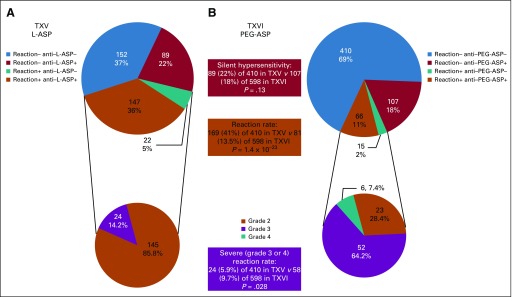
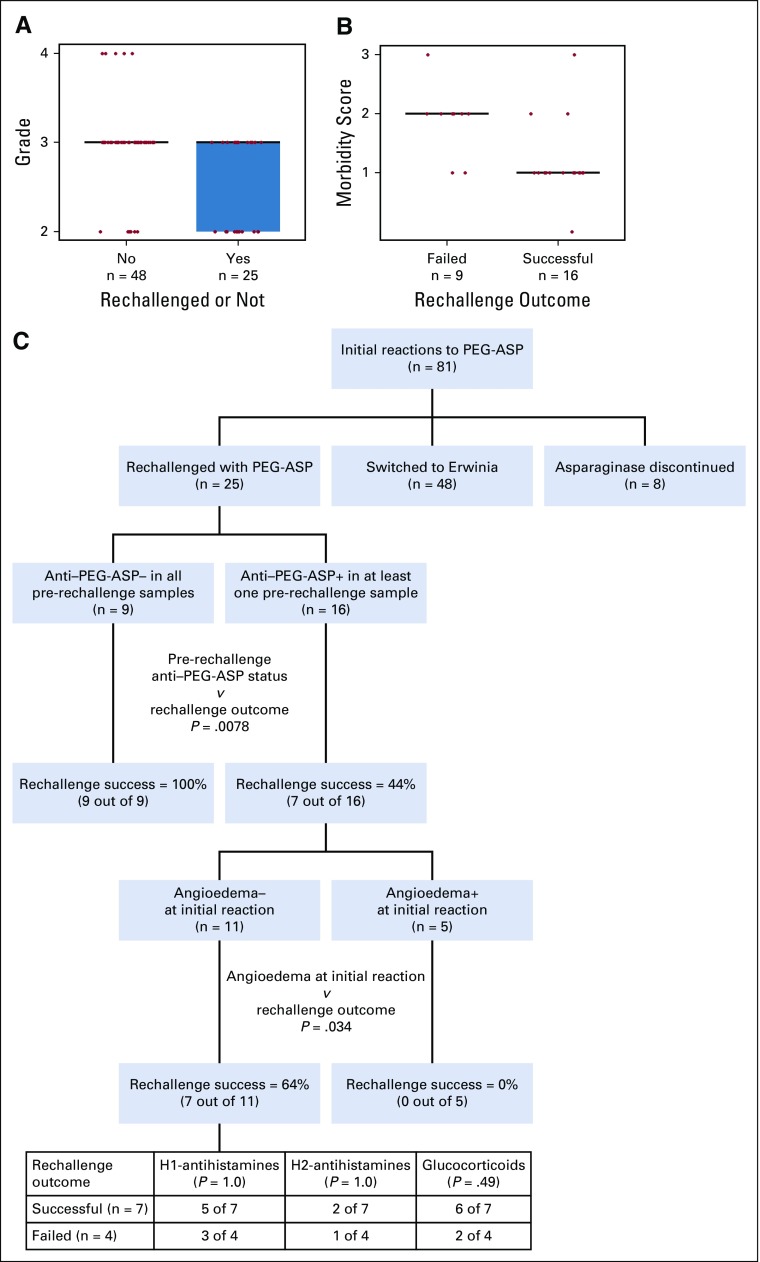
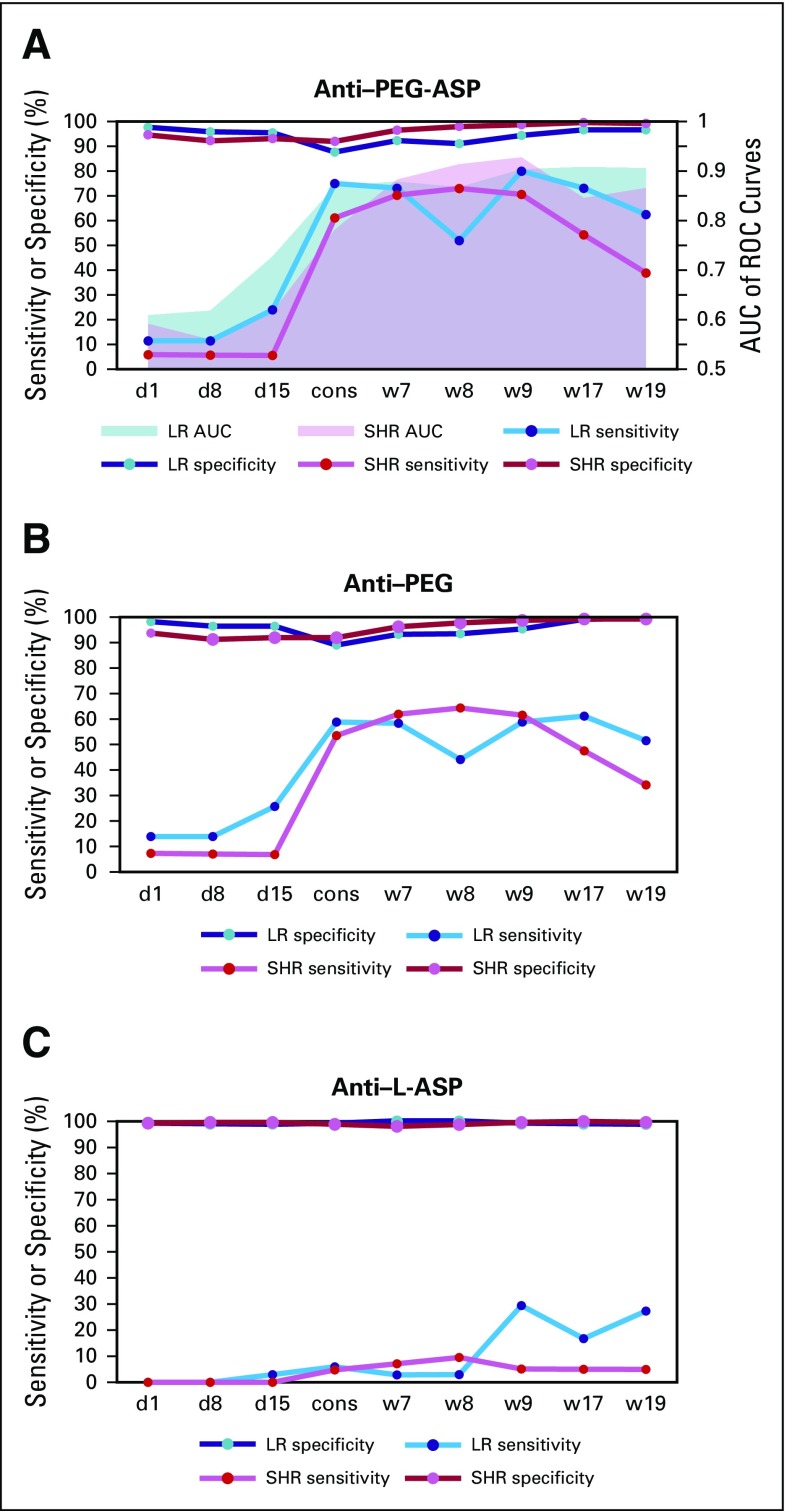
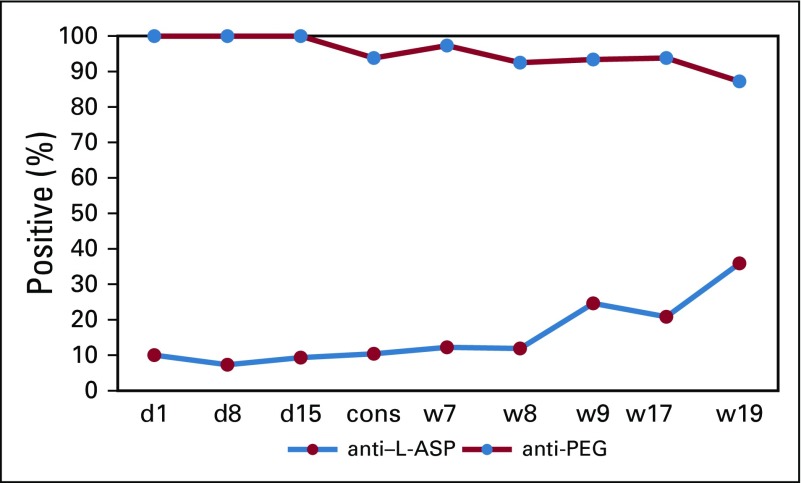
Results: Grade 2 to 4 reactions were less common in the Total XVI study with PEG-ASP (81 [13.5%] of 598) than in the Total XV study with L-ASP (169 [41.2%] of 410; P = 1.4 × 10-23). For Total XVI, anti-PEG, not anti-L-ASP, was the predominant component of anti-PEG-ASP antibodies (96%). In a multivariable analysis, more intrathecal therapy (IT) predicted fewer reactions (P = 2.4 × 10-5), which is consistent with an immunosuppressant contribution of IT. Anti-PEG-ASP was associated with accelerated drug clearance (P = 5.0 × 10-6). Failure of rechallenge after initial reactions was associated with anti-PEG-ASP (P = .0078) and was predicted by the occurrence of angioedema with first reaction (P = .01).
Conclusion: Less IT therapy was the only independent clinical risk factor for reactions to PEG-ASP. PEG, and not L-ASP, is the major antigen that causes allergic reactions. Anti-PEG-ASP has utility in predicting and confirming clinical reactions to PEG-ASP as well as in identifying patients who are most likely to experience failure with rechallenge.
Figures
Comment in
-
Native E. coli asparaginase upfront should be replaced by PEGasparaginase upfront in the treatment of pediatric patients with acute lymphoblastic leukemia.Hematol Oncol. 2022 Oct;40(4):809-811. doi: 10.1002/hon.2960. Epub 2022 Jan 2. Hematol Oncol. 2022. PMID: 34961954 No abstract available.
References
-
- Mishra P, Nayak B, Dey RK. PEGylation in anti-cancer therapy: An overview. Asian Journal of Pharmaceutical Sciences. 2016;11:337–348.
-
- Advani AS, Sanford B, Luger S, et al. Frontline-treatment of acute lymphoblastic leukemia (ALL) in older adolescents and young adults (AYA) using a pediatric regimen is feasible: Toxicity results of the prospective US Intergroup Trial C10403 (Alliance) Blood. 2013;122:3903.
-
- Pieters R, de Groot-Kruseman H, Van der Velden V, et al. Successful therapy reduction and intensification for childhood acute lymphoblastic leukemia based on minimal residual disease monitoring: Study ALL10 from the Dutch Childhood Oncology Group. J Clin Oncol. 2016;34:2591–2601. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
