

doi: 10.5935/abc.20190075.
Brazilian Fetal Cardiology Guidelines - 2019
[Article in
English,
Portuguese]
Affiliations
- PMID: 31188968
- PMCID: PMC6555576
- DOI: 10.5935/abc.20190075
Item in Clipboard
Brazilian Fetal Cardiology Guidelines - 2019
[Article in
English,
Portuguese]
Arq Bras Cardiol.
.
No abstract available
Figures
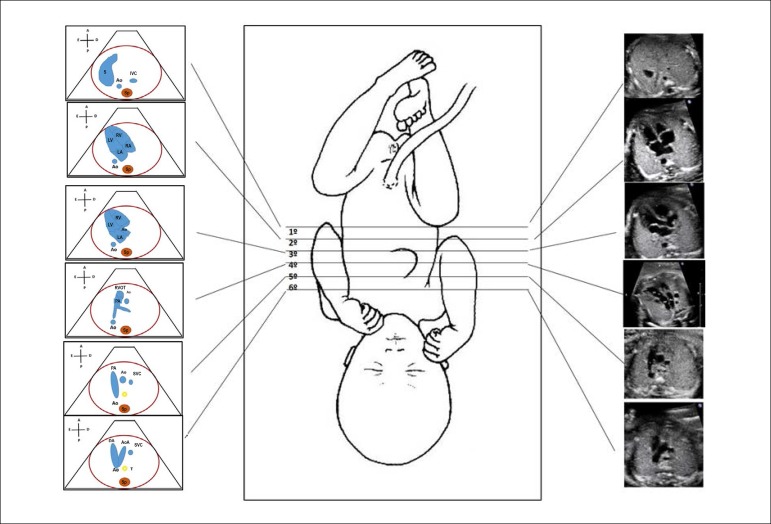
Standardization of fetal heart screening, scanning the fetal vessels
and heart from the infradiaphragmatic region towards the cranium.
There are 6 levels, being the first exactly below the diaphragm,
which allows the identification of the descending aorta and inferior
vena cava; second, the four-chamber view; third, left ventricular
outflow tract; fourth, right ventricular outflow tract; fifth, three
vessel view, and, sixth, three vessel and trachea view. Ao: Aorta; AoA: aortic arch; Asc: ascending; DA: ductus arteriosus;
IVC: inferior vena cava; LA: left atrium; LV: left ventricle; PA:
pulmonary artery; RA: right atrium; RV: right ventricle; RVOT: right
ventricular outflow tract; S: stomach; Sp: spine; SVC: superior vena
cava; T: trachea.
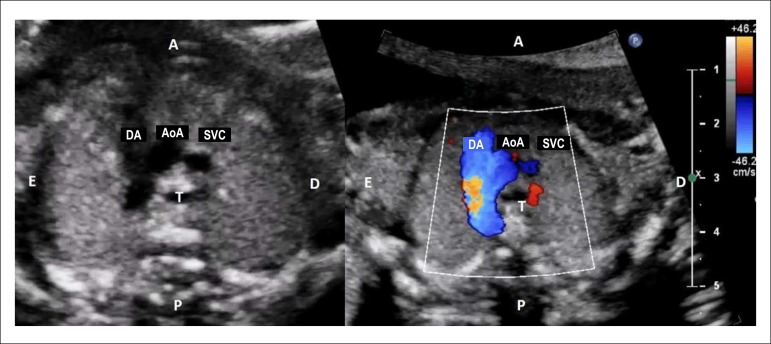
Aorta and pulmonary artery appear elongated, going toward the
descending aorta. Both converge to the aorta forming an image
similar to a V letter. The trachea is to the right of the aortic
arch, demonstrating that the latter descends to the left. During
color flow mapping, both arches are observed to have flow in the
same direction, i.e., from the heart toward the descending
thoracic aorta. AoA: aortic arch; DA: ductal arch; SVC: superior vena cava; T:
trachea.

Long axis view of the aortic arch. The shape of the aortic arch is
similar to a cane.

Longitudinal plane slightly anterior and to the left of the fetus,
showing the long axis view of the ductal arch. The ductal arch has a
different angle than the aortic and looks like a golf club. LPA: left pulmonary artery; PA: pulmonary artery.
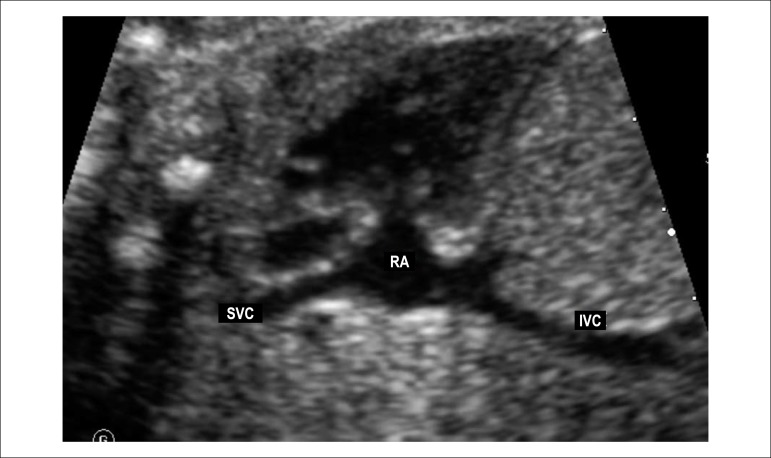
Longitudinal fetal plane tilting posteriorly, showing the bicaval
view. IVC: inferior vena cava; RA: right atrium; SVC: superior vena
cava.

Short-axis of the ventricles. In this plane it is possible to analyze
the position of the papillary muscles of the right and left
ventricles. It is also of great utility in detecting subtler forms
of atrioventricular septal defect when it is presented with two
valvular orifices. A: anterior; P: posterior; LV: left ventricle; RV: right ventricle;
S: stomach.
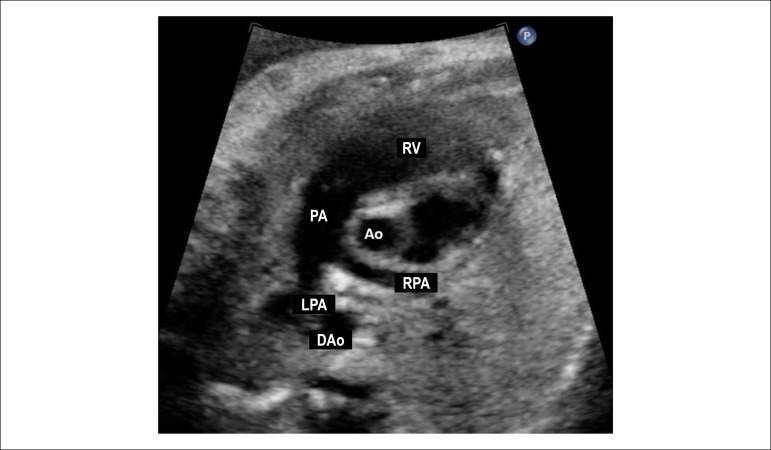
Short axis view of the great vessels. This plane shows the
relationship between the great arteries, with the aorta being in the
center of the heart and posteriorly and the right ventricular
outflow tract surrounding the aorta anteriorly. This is an excellent
plane for identifying perimembranous ventricular septal defects and
pulmonary obstructions due to the anterior deviation of the
infundibular septum observed in the tetralogy of Fallot. Ao: aorta; DAo: descending aorta; LPA: left pulmonary artery; PA:
pulmonary artery; RPA: right pulmonary artery; RV: right
ventricle.
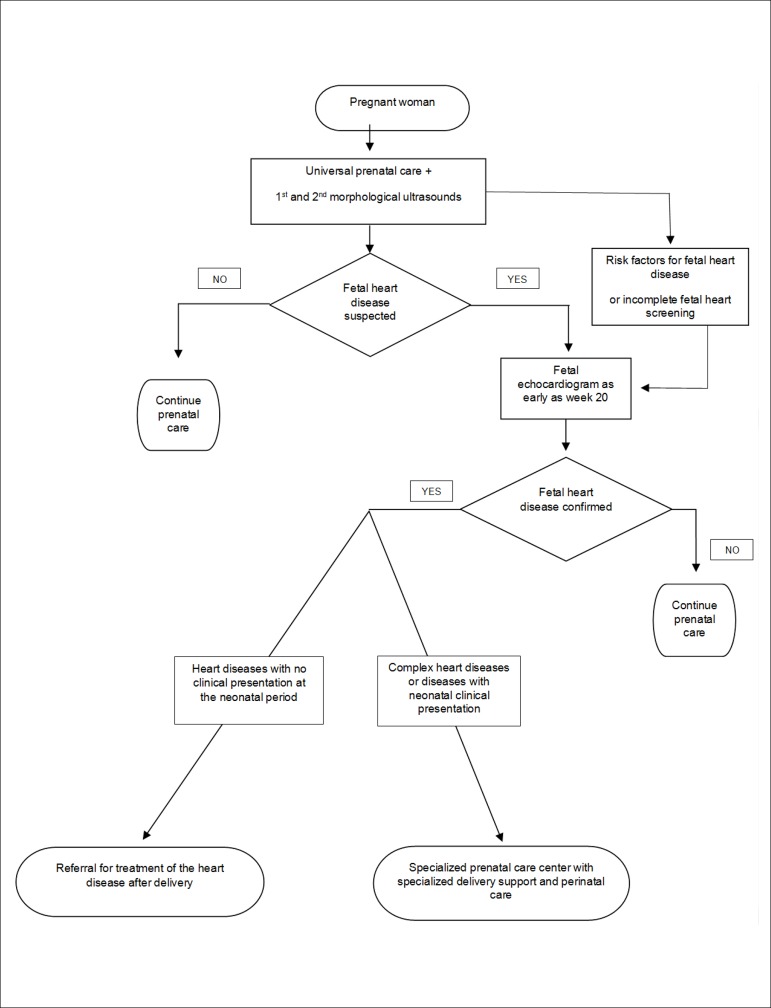
Fetal care flowchart according to the specific fetal heart condition. USG: ultrasound.
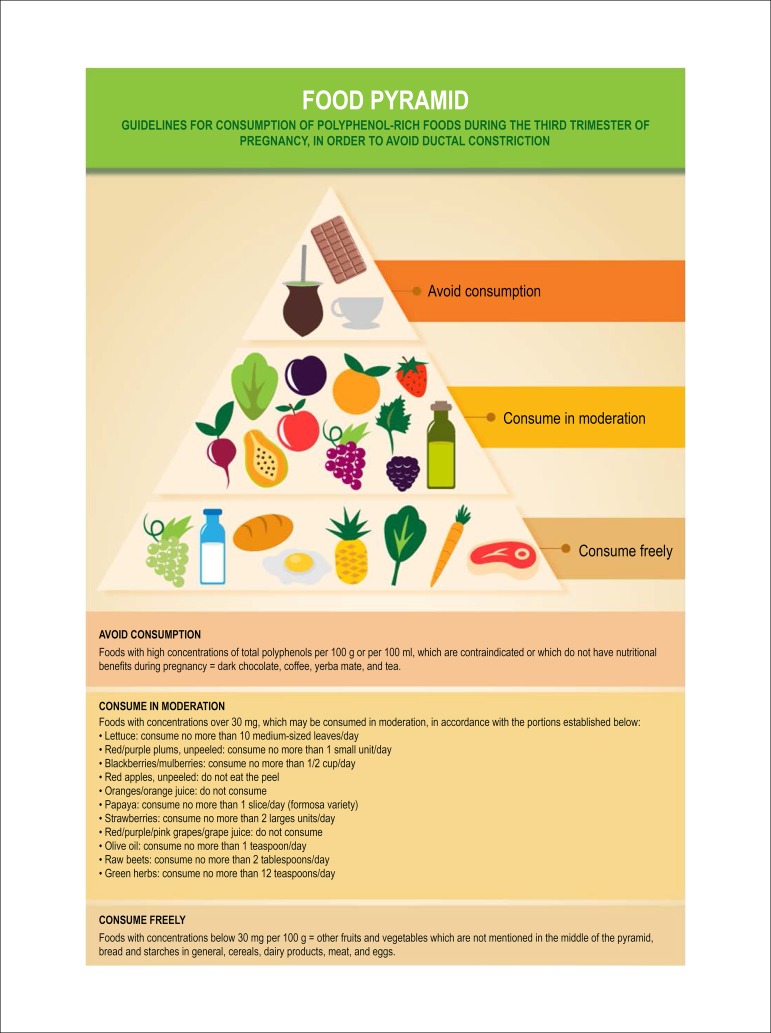
Food pyramid.
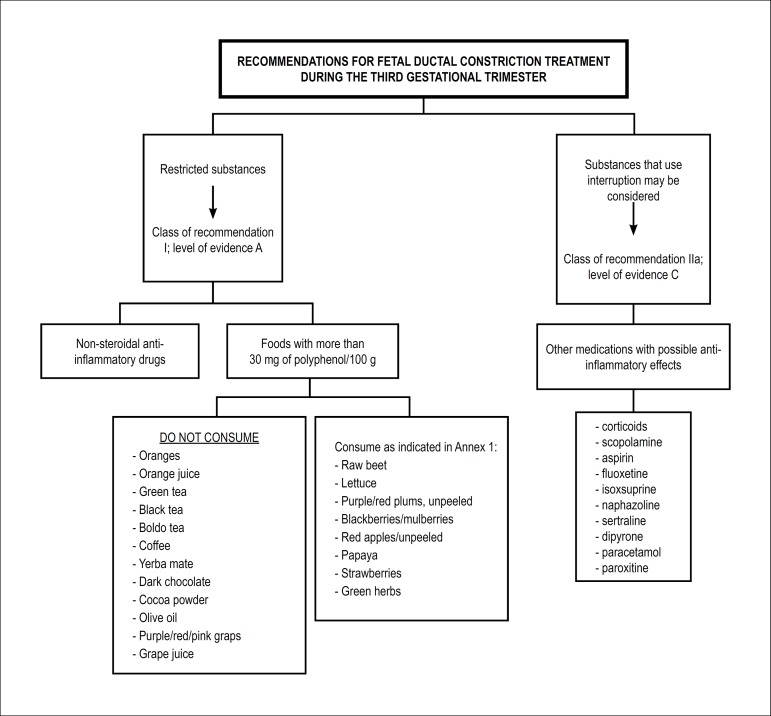
Recommendations for fetal ductal constriction treatment during
the third gestational trimester. In cases in which there is no reversal of the ductal constriction
and its consequences after initiation of treatment, preterm
delivery may be considered, since fetal pulmonary maturity has
been established. Class of recommendation: IIb; Level of
evidence: C.
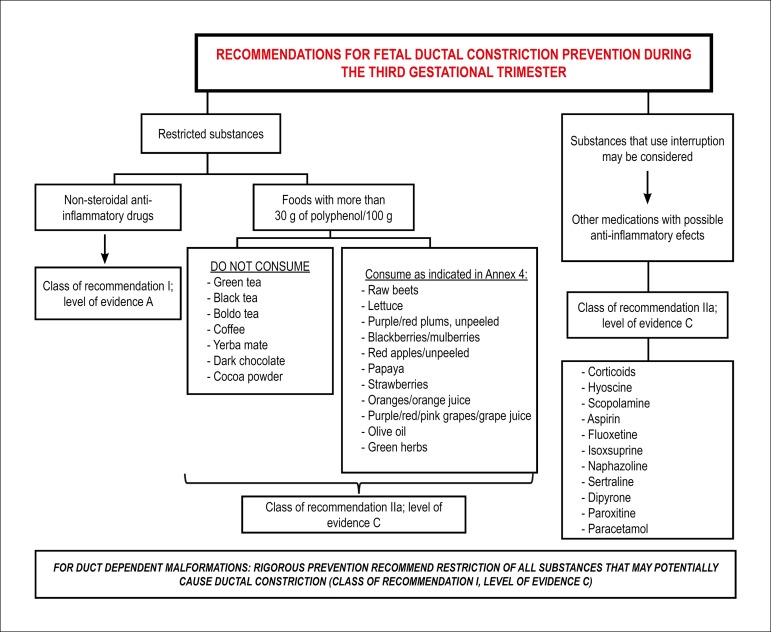
Recommendations for fetal ductal constriction prevention during
the third gestational trimester.
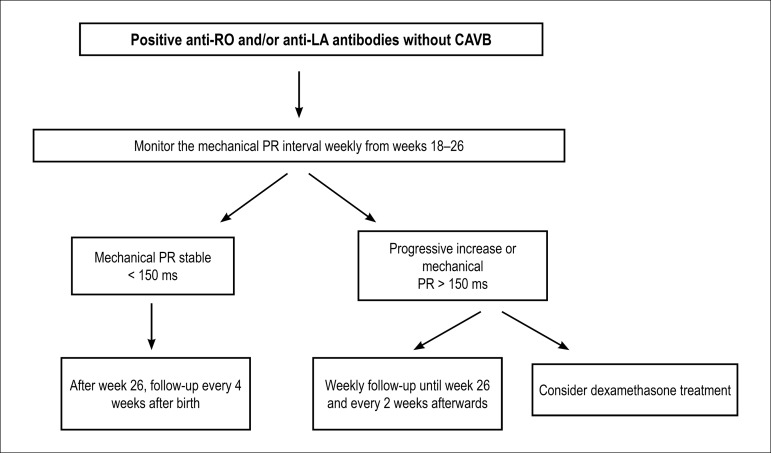
Suggested approach for pregnant women with positive antibodies,
without fetal CAVB. CAVB: complete atrioventricular block; ms: miliseconds.
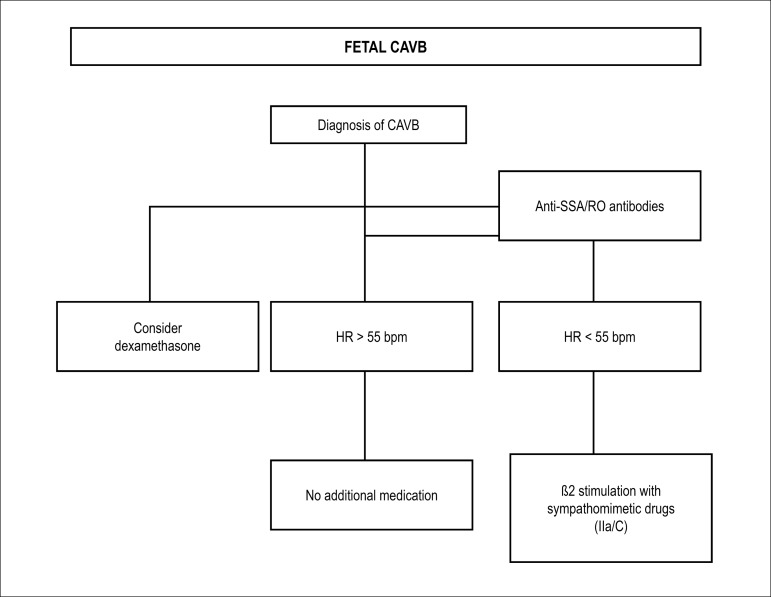
Suggested approach for fetuses who have CAVB. CAVB: complete atrioventricular block; HR: heart rate.
Sinus tachycardia clinical management.
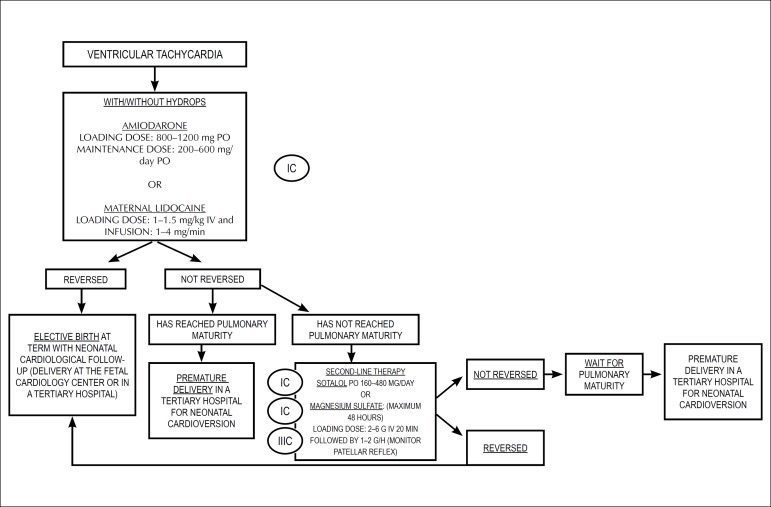
Treatment flowchart for ventricular tachycardia. IV: intravenous; PO: orally.
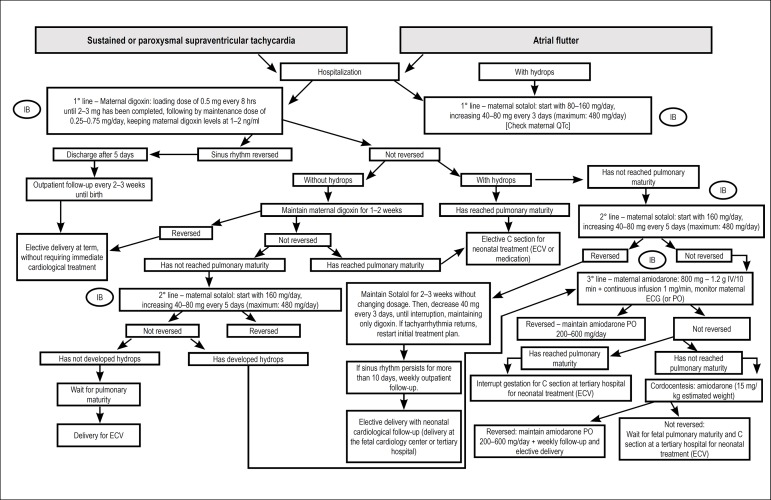
Flowchart treatment for supraventricular tachycardias. ECV: electric cardioversion; IV: intravenous; PO: orally.
Similar articles
-
[Fetal cardiac disorders].Schweiz Med Wochenschr. 1995 Feb 18;125(7):294-303. Schweiz Med Wochenschr. 1995. PMID: 7878408 Review. French.
-
Isolated major congenital heart disease.Ultrasound Obstet Gynecol. 2001 May;17(5):370-9. doi: 10.1046/j.1469-0705.2001.00439.x. Ultrasound Obstet Gynecol. 2001. PMID: 11380959 No abstract available.
-
[Left heart hypoplasia: diagnosis and current obstetrical management. Apropos of 4 cases].J Gynecol Obstet Biol Reprod (Paris). 1994;23(4):425-31. J Gynecol Obstet Biol Reprod (Paris). 1994. PMID: 8051372 French. No abstract available.
-
[Fetal cardiology].Arch Pediatr. 2004 Jun;11(6):637-8. doi: 10.1016/j.arcped.2004.03.115. Arch Pediatr. 2004. PMID: 15158864 French. No abstract available.
-
Cardiac ultrasound: its role in the recognition and management of fetal heart disease.Echocardiography. 1991 Jul;8(4):441-66. doi: 10.1111/j.1540-8175.1991.tb01006.x. Echocardiography. 1991. PMID: 10149265 Review.
Cited by
-
Congenital heart disease: epidemiological profile of live births, geographical distribution and temporal trends in Brazil from 2012 to 2022.BMC Cardiovasc Disord. 2025 Aug 11;25(1):599. doi: 10.1186/s12872-025-05079-8. BMC Cardiovasc Disord. 2025. PMID: 40790621 Free PMC article.
-
Development of a Z-score equation for atrioventricular interval measurement by two-dimensional pulsed Doppler echocardiography in normal fetuses between 16 and 33+6 weeks of gestation.Ultrasonography. 2025 May;44(3):212-219. doi: 10.14366/usg.24142. Epub 2025 Apr 30. Ultrasonography. 2025. PMID: 40360248 Free PMC article.
-
Inappropriate fetal sinus tachycardia at 9 weeks of gestation.Ann Pediatr Cardiol. 2022 Jul-Aug;15(4):399-403. doi: 10.4103/apc.apc_130_21. Epub 2023 Jan 6. Ann Pediatr Cardiol. 2022. PMID: 36935829 Free PMC article.
-
Epicardial pacing lead implantation for congenital complete atrioventricular block immediately after birth: a case report.J Med Case Rep. 2023 Nov 1;17(1):453. doi: 10.1186/s13256-023-04190-8. J Med Case Rep. 2023. PMID: 37907974 Free PMC article.
-
Effects of Cocoa Consumption on Cardiometabolic Risk Markers: Meta-Analysis of Randomized Controlled Trials.Nutrients. 2024 Jun 18;16(12):1919. doi: 10.3390/nu16121919. Nutrients. 2024. PMID: 38931273 Free PMC article.
References
-
- Allan LD, Sharland GK, Milburn A, Lockhart SM, Groves AM, Anderson RH, et al. Prospective diagnosis of 1006 consecutive cases of congenital heart disease in the fetus. J Am Coll Cardiol. 1994;23(6):1452–1458. - PubMed
-
- Brick DH, Allan LD. Outcome of prenatally diagnosed congenital heart disease: an update. Pediatr Cardiol. 2002;23(4):449–453. - PubMed
-
- Nomura RM, Brizot ML, Liao AW, Hernandez WR, Zugaib M. Conjoined twins and legal authorization for abortion. Rev Assoc Med Bras (1992) 2011;57(2):205–210. - PubMed
-
- Ewigman BG, Crane JP, Frigoletto FD, LeFevre ML, Bain RP, McNellis D. Effect of prenatal ultrasound screening on perinatal outcome: RADIUS Study Group. N Engl J Med. 1993;329(12):821–827. - PubMed
-
- Tegnander E, Eik-Nes SH, Johansen OJ, Linker DT. Prenatal detectionof heart defects at the routine fetal examination at 18 weeks in a nonselectedpopulation. Ultrasound Obstet Gynecol. 1995;5(6):372–380. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
