

Clinical Metagenomic Sequencing for Diagnosis of Meningitis and Encephalitis
- PMID: 31189036
- PMCID: PMC6764751
- DOI: 10.1056/NEJMoa1803396
Clinical Metagenomic Sequencing for Diagnosis of Meningitis and Encephalitis
Abstract
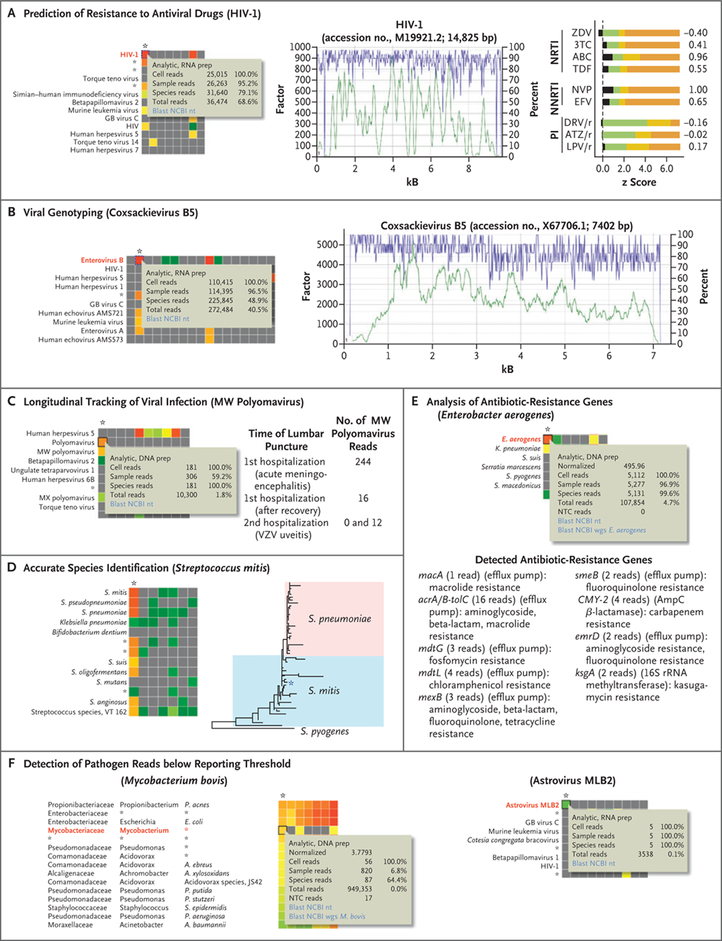
Background: Metagenomic next-generation sequencing (NGS) of cerebrospinal fluid (CSF) has the potential to identify a broad range of pathogens in a single test.
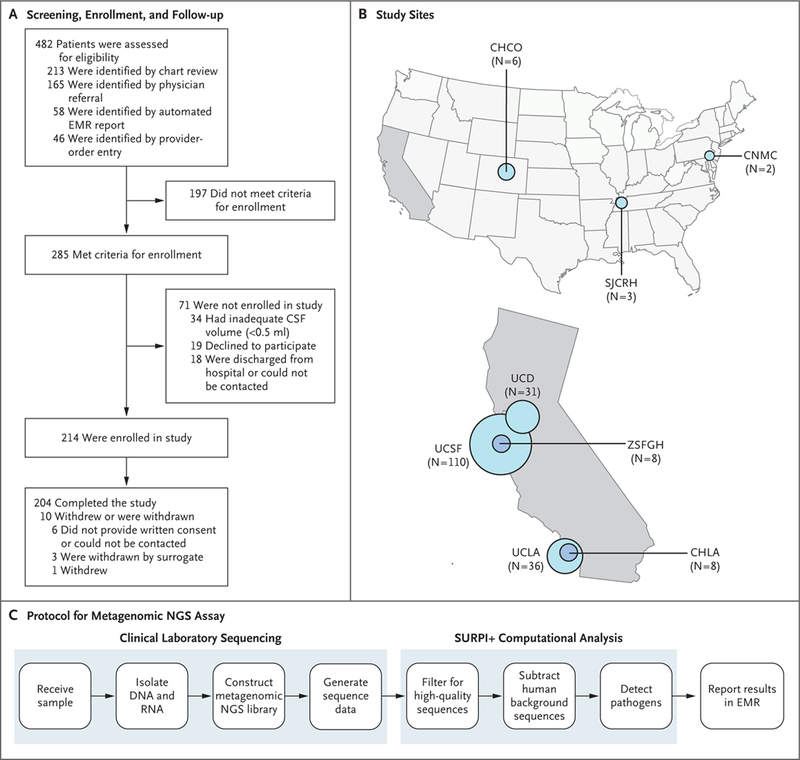
Methods: In a 1-year, multicenter, prospective study, we investigated the usefulness of metagenomic NGS of CSF for the diagnosis of infectious meningitis and encephalitis in hospitalized patients. All positive tests for pathogens on metagenomic NGS were confirmed by orthogonal laboratory testing. Physician feedback was elicited by teleconferences with a clinical microbial sequencing board and by surveys. Clinical effect was evaluated by retrospective chart review.
Results: We enrolled 204 pediatric and adult patients at eight hospitals. Patients were severely ill: 48.5% had been admitted to the intensive care unit, and the 30-day mortality among all study patients was 11.3%. A total of 58 infections of the nervous system were diagnosed in 57 patients (27.9%). Among these 58 infections, metagenomic NGS identified 13 (22%) that were not identified by clinical testing at the source hospital. Among the remaining 45 infections (78%), metagenomic NGS made concurrent diagnoses in 19. Of the 26 infections not identified by metagenomic NGS, 11 were diagnosed by serologic testing only, 7 were diagnosed from tissue samples other than CSF, and 8 were negative on metagenomic NGS owing to low titers of pathogens in CSF. A total of 8 of 13 diagnoses made solely by metagenomic NGS had a likely clinical effect, with 7 of 13 guiding treatment.
Conclusions: Routine microbiologic testing is often insufficient to detect all neuroinvasive pathogens. In this study, metagenomic NGS of CSF obtained from patients with meningitis or encephalitis improved diagnosis of neurologic infections and provided actionable information in some cases. (Funded by the National Institutes of Health and others; PDAID ClinicalTrials.gov number, NCT02910037.).
Copyright © 2019 Massachusetts Medical Society.
Conflict of interest statement
Disclosure forms provided by the authors are available with the full text of this article at
Figures

References
-
- Glaser CA, Gilliam S, Schnurr D, et al. In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998–2000. Clin Infect Dis 2003; 36: 731–42. - PubMed
-
- Glaser CA, Honarmand S, Anderson LJ, et al. Beyond viruses: clinical profiles and etiologies associated with encephalitis. Clin Infect Dis 2006; 43: 1565–77. - PubMed
-
- Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis 2010; 10: 835–44. - PubMed
-
- Khetsuriani N, Holman RC, Anderson LJ. Burden of encephalitis-associated hospitalizations in the United States, 1988–1997. Clin Infect Dis 2002; 35: 175–82. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical