

Diagnosis of obstructive coronary artery disease using computed tomography angiography in patients with stable chest pain depending on clinical probability and in clinically important subgroups: meta-analysis of individual patient data
- PMID: 31189617
- PMCID: PMC6561308
- DOI: 10.1136/bmj.l1945
Diagnosis of obstructive coronary artery disease using computed tomography angiography in patients with stable chest pain depending on clinical probability and in clinically important subgroups: meta-analysis of individual patient data
Abstract
Objective: To determine whether coronary computed tomography angiography (CTA) should be performed in patients with any clinical probability of coronary artery disease (CAD), and whether the diagnostic performance differs between subgroups of patients.
Design: Prospectively designed meta-analysis of individual patient data from prospective diagnostic accuracy studies.
Data sources: Medline, Embase, and Web of Science for published studies. Unpublished studies were identified via direct contact with participating investigators.
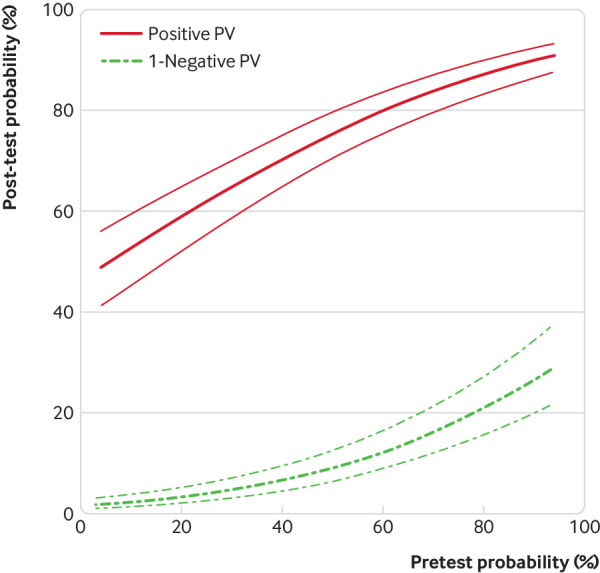
Eligibility criteria for selecting studies: Prospective diagnostic accuracy studies that compared coronary CTA with coronary angiography as the reference standard, using at least a 50% diameter reduction as a cutoff value for obstructive CAD. All patients needed to have a clinical indication for coronary angiography due to suspected CAD, and both tests had to be performed in all patients. Results had to be provided using 2×2 or 3×2 cross tabulations for the comparison of CTA with coronary angiography. Primary outcomes were the positive and negative predictive values of CTA as a function of clinical pretest probability of obstructive CAD, analysed by a generalised linear mixed model; calculations were performed including and excluding non-diagnostic CTA results. The no-treat/treat threshold model was used to determine the range of appropriate pretest probabilities for CTA. The threshold model was based on obtained post-test probabilities of less than 15% in case of negative CTA and above 50% in case of positive CTA. Sex, angina pectoris type, age, and number of computed tomography detector rows were used as clinical variables to analyse the diagnostic performance in relevant subgroups.
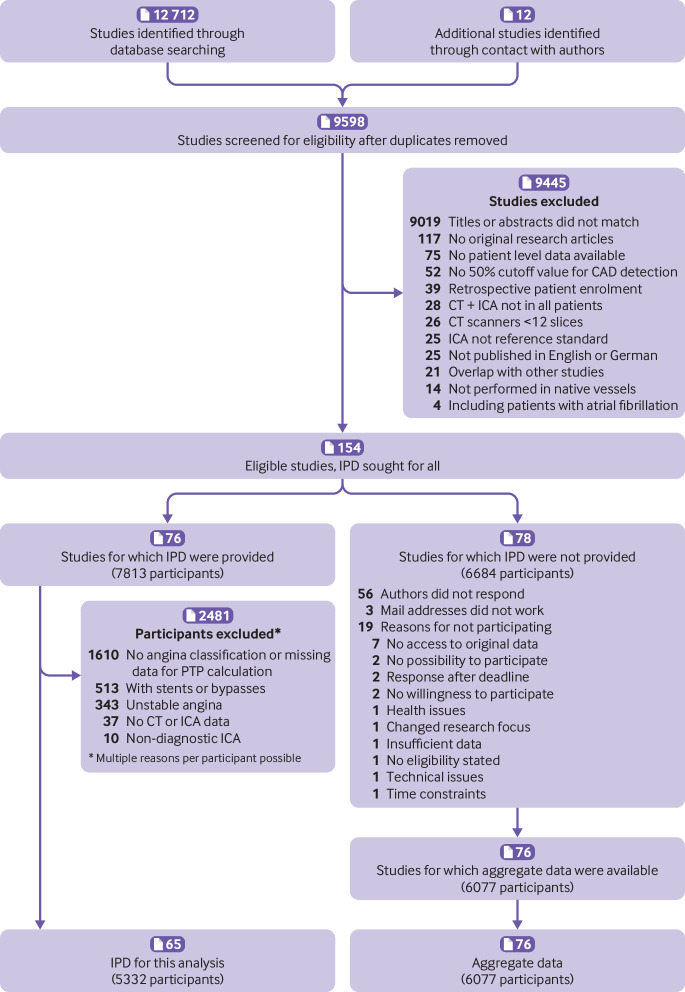
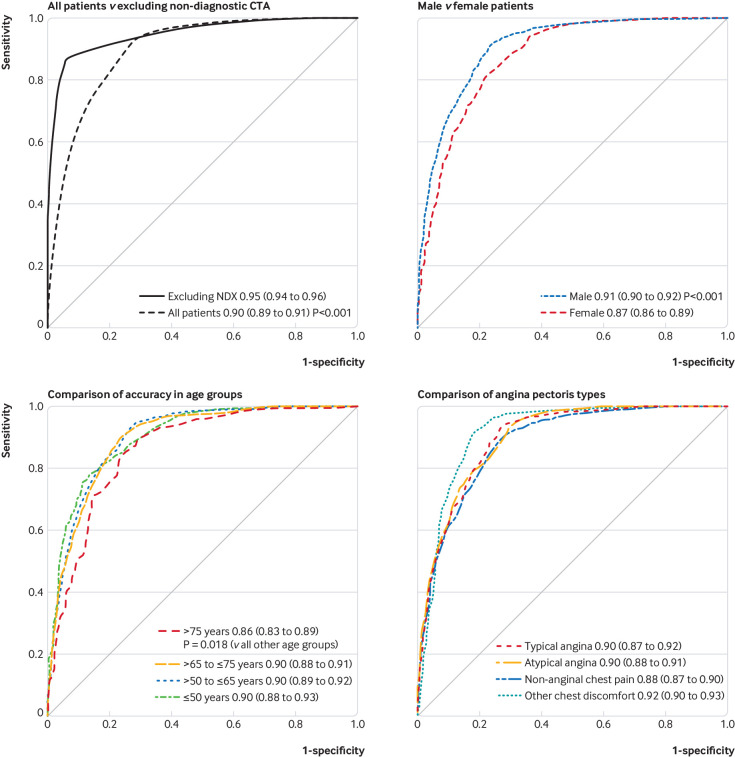
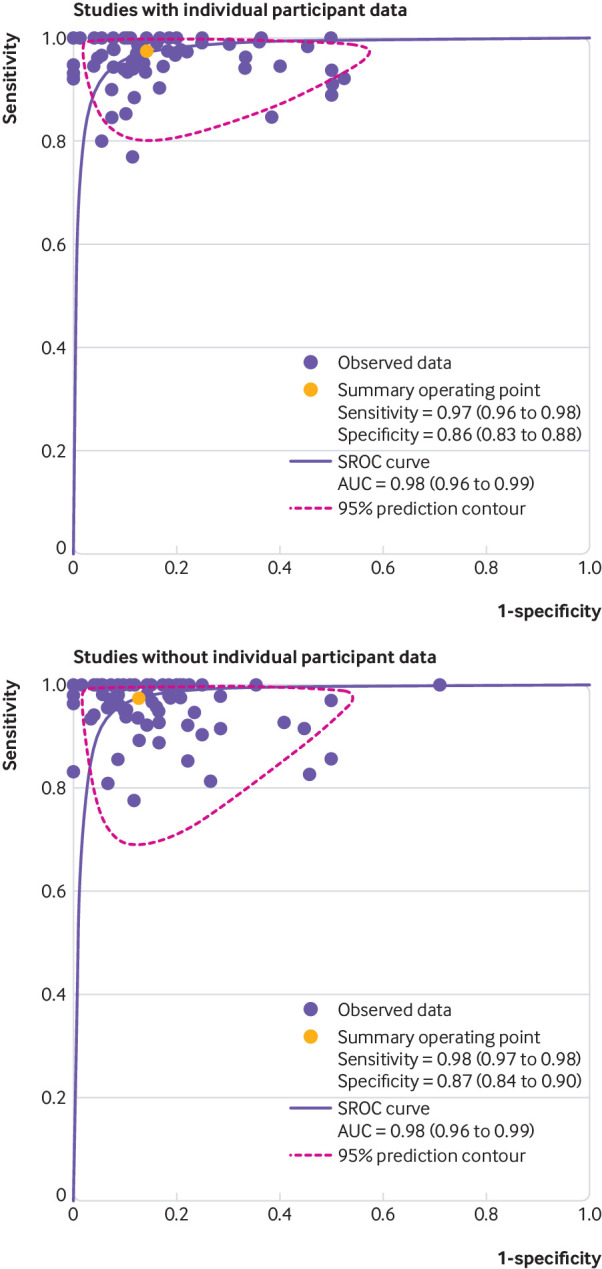
Results: Individual patient data from 5332 patients from 65 prospective diagnostic accuracy studies were retrieved. For a pretest probability range of 7-67%, the treat threshold of more than 50% and the no-treat threshold of less than 15% post-test probability were obtained using CTA. At a pretest probability of 7%, the positive predictive value of CTA was 50.9% (95% confidence interval 43.3% to 57.7%) and the negative predictive value of CTA was 97.8% (96.4% to 98.7%); corresponding values at a pretest probability of 67% were 82.7% (78.3% to 86.2%) and 85.0% (80.2% to 88.9%), respectively. The overall sensitivity of CTA was 95.2% (92.6% to 96.9%) and the specificity was 79.2% (74.9% to 82.9%). CTA using more than 64 detector rows was associated with a higher empirical sensitivity than CTA using up to 64 rows (93.4% v 86.5%, P=0.002) and specificity (84.4% v 72.6%, P<0.001). The area under the receiver-operating-characteristic curve for CTA was 0.897 (0.889 to 0.906), and the diagnostic performance of CTA was slightly lower in women than in with men (area under the curve 0.874 (0.858 to 0.890) v 0.907 (0.897 to 0.916), P<0.001). The diagnostic performance of CTA was slightly lower in patients older than 75 (0.864 (0.834 to 0.894), P=0.018 v all other age groups) and was not significantly influenced by angina pectoris type (typical angina 0.895 (0.873 to 0.917), atypical angina 0.898 (0.884 to 0.913), non-anginal chest pain 0.884 (0.870 to 0.899), other chest discomfort 0.915 (0.897 to 0.934)).
Conclusions: In a no-treat/treat threshold model, the diagnosis of obstructive CAD using coronary CTA in patients with stable chest pain was most accurate when the clinical pretest probability was between 7% and 67%. Performance of CTA was not influenced by the angina pectoris type and was slightly higher in men and lower in older patients.
Systematic review registration: PROSPERO CRD42012002780.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: PS and MD had support from the joint programme of the German Research Foundation and the German Federal Ministry of Education and Research for the submitted work; PS has support from the German Research Foundation, grants from the European Union and grants from Bayer Pharma AG; GP reports grants from General Electric and is on the speakers bureau for Medtronic and Bracco; JH is on the speakers bureau for Abbott Vascular and Edwards Life Sciences; BG reports that the Cliniques St Luc UCL holds a master research agreement with Philips Medical Systems; UJS reports institutional grants, personal fees, and non-financial support from Astellas, Bayer, General Electric, Guerbet, HeartFlow, and Siemens; BLN reports grants from Siemens and HeartFlow, JKreports grants from CardiRad and personal fees from GE Healthcare; RRB reports that the University Hospital Zurich holds a research agreement with GE Healthcare; MYC reports an institutional research agreement with Canon Medical, formerly Toshiba Medical (no financial support/funding); DAH reports institutional support from Philips Healthcare during the conduct of the primary study; BH-M reports that the University Hospital Zurich holds a research agreement with GE Healthcare; BJC reports grants from CV Diagnostix and non-financial support from TeraRecon during the conduct of the study; PAK reports that the University Hospital Zurich holds a research agreement with GE Healthcare; KFK reports grants from Toshiba Medical Corporation, grants from the Danish Heart Foundation, grants from AP Møller og hustru Chastine McKinney Møllers Fond, and grants from the Danish Agency for Science, Technology and Innovation by the Danish Council for Strategic Research; AA-Z reports grants and non-financial support from Toshiba Medical Systems; JH reports grants from Toshiba Medical Systems during the conduct of the study; AS reports personal fees from General Electric and Toshiba; NP is on the speakers bureau for Toshiba Medical Systems and reports grants from Toshiba Medical Systems; GMS reports grants from the German Federal Ministry of Education and Research (BMBF), during the conduct of the study; DEN reports grants from Toshiba Medical Systems; MD is supported by the FP7 programme of the European Commission for the randomised multicentre DISCHARGE trial (603266-2, HEALTH-2012.2.4.-2) from the Heisenberg programme of the German Research Foundation (DE 1361/14-1), and the Digital Health Accelerator of the Berlin Institute of Health, has received lecture fees from Canon Medical Systems, Guerbet, Cardiac MR Academy Berlin, and Bayer, is the editor of Cardiac CT (Springer), and offers hands-on workshops on cardiac CT imaging (http://herz-kurs.de/); Charité institutional master research agreements exist with Siemens Medical Solutions, General Electric, Philips Medical Systems, and Canon Medical Systems, and the terms of these arrangements are managed by the legal department of Charité - Universitätsmedizin Berlin.
Figures
References
-
- Montalescot G, Sechtem U, Achenbach S, et al. Task Force Members. ESC Committee for Practice Guidelines. Document Reviewers 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949-3003. 10.1093/eurheartj/eht296 - DOI - PubMed
-
- National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. Secondary chest pain of recent onset: assessment and diagnosis 2016. https://www.nice.org.uk/guidance/cg95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous