

The Current Status of Intervention for Intermediate Coronary Stenosis in the Korean Percutaneous Coronary Intervention (K-PCI) Registry
- PMID: 31190480
- PMCID: PMC6813154
- DOI: 10.4070/kcj.2019.0074
The Current Status of Intervention for Intermediate Coronary Stenosis in the Korean Percutaneous Coronary Intervention (K-PCI) Registry
Abstract
Background and objectives: Intermediate coronary lesion that can be under- or over-estimated by visual estimation frequently results in stenting of functionally nonsignificant lesions or deferral of percutaneous coronary intervention (PCI) of significant lesions inappropriately. We evaluated current status of PCI for intermediate lesions from a standardized database in Korea.
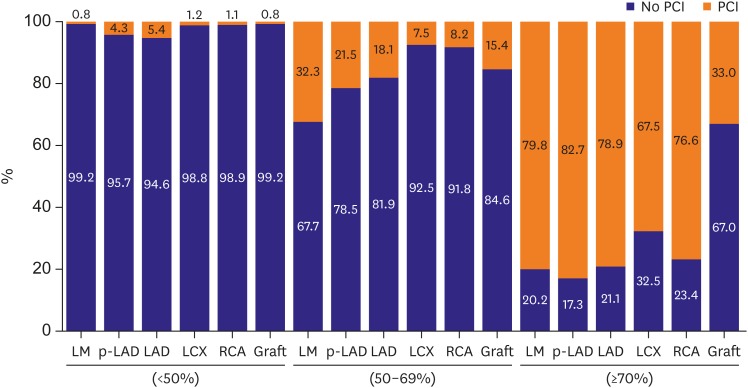
Methods: We analyzed the Korean percutaneous coronary intervention (K-PCI) registry data which collected a standardized PCI database of the participating hospitals throughout the country from January 1, 2014, through December 31, 2014. Intermediate lesion was defined as a luminal narrowing between 50% and 70% by visual estimation and then compared whether the invasive physiologic or imaging study was performed or not.
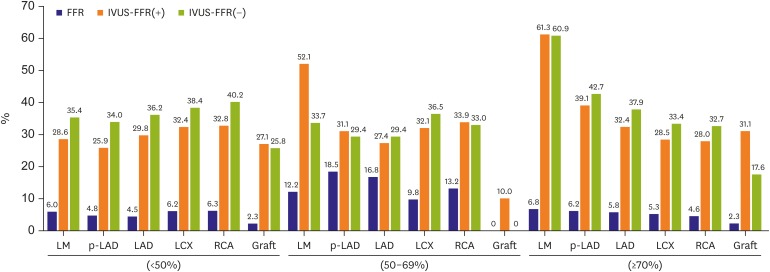
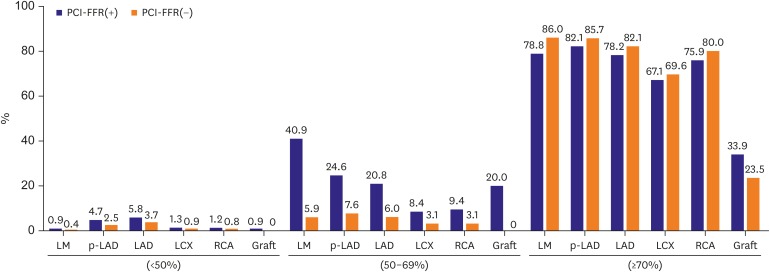
Results: Physiology-guided PCI for intermediate lesions was performed in 16.8% for left anterior descending artery (LAD), 9.8% for left circumflex artery (LCX), 13.2% for right coronary artery (RCA). PCI was more frequently performed using intravascular ultrasound (IVUS) than using fractional flow reserve (FFR) for coronary artery segments (27.7% vs. 13.9% for LAD, 32.9% vs. 8.1% for LCX, and 33.8% vs. 10.8% for RCA). In accordance with or without FFR, PCI for intermediate lesions was more frequently performed in the hospitals with available FFR device than without FFR, especially in left main artery (LM), proximal LAD lesion (40.9% vs. 5.9% for LM, 24.6% vs 7.6% for proximal LAD).
Conclusions: These data provide the current PCI practice pattern with the use of FFR and IVUS in intermediate lesion. More common use of FFR for intermediate lesion should be encouraged.
Keywords: Coronary artery disease; Fractional flow reserve, myocardial; Percutaneous coronary intervention.
Copyright © 2019. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Park SJ, Kang SJ, Ahn JM, et al. Visual-functional mismatch between coronary angiography and fractional flow reserve. JACC Cardiovasc Interv. 2012;5:1029–1036. - PubMed
-
- Trask N, Califf RM, Conley MJ, et al. Accuracy and interobserver variability of coronary cineangiography: a comparison with postmortem evaluation. J Am Coll Cardiol. 1984;3:1145–1154. - PubMed
-
- Katritsis D, Webb-Peploe M. Limitations of coronary angiography: an underestimated problem? Clin Cardiol. 1991;14:20–24. - PubMed
-
- Patel MR, Calhoon JH, Dehmer GJ, et al. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 appropriate use criteria for coronary revascularization in patients with stable ischemic heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2017;69:2212–2241. - PubMed
-
- Authors/Task Force members. Windecker S, Kolh P, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) Eur Heart J. 2014;35:2541–2619. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
