

Implementation of a Clostridioides difficile prevention bundle: Understanding common, unique, and conflicting work system barriers and facilitators for subprocess design
- PMID: 31190669
- PMCID: PMC7212912
- DOI: 10.1017/ice.2019.150
Implementation of a Clostridioides difficile prevention bundle: Understanding common, unique, and conflicting work system barriers and facilitators for subprocess design
Abstract
Objective: Clostridioides difficile (C. difficile) poses a major challenge to the healthcare system. We assessed factors that should be considered when designing subprocesses of a C. difficile infection (CDI) prevention bundle.
Design: Phenomenological qualitative study.
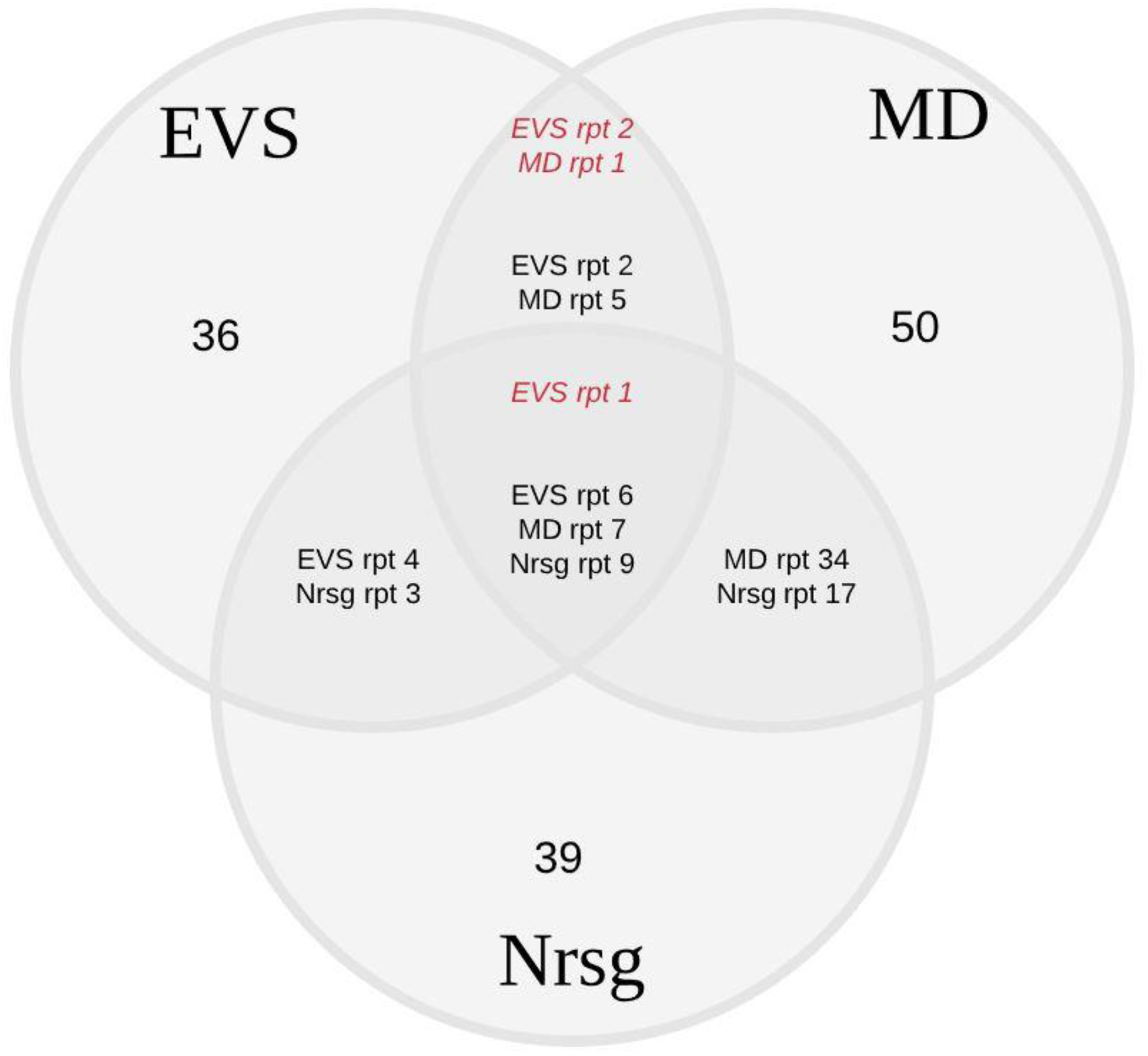
Methods: We conducted 3 focus groups of environmental services (EVS) staff, physicians, and nurses to assess their perspectives on a CDI prevention bundle. We used the Systems Engineering Initiative for Patient Safety (SEIPS) model to examine 5 subprocesses of the CDI bundle: diagnostic testing, empiric isolation, contact isolation, hand hygiene, and environmental disinfection. We coded transcripts to the 5 SEIPS elements and ensured scientific rigor. We sought to determine common, unique, and conflicting factors across stakeholder groups and subprocesses of the CDI bundle.
Results: Each focus group lasted 1.5 hours on average. Common work-system barriers included inconsistencies in knowledge and practice of CDI management procedures; increased workload; poor setup of aspects of the physical environment (eg, inconvenient location of sinks); and inconsistencies in CDI documentation. Unique barriers and facilitators were related to specific activities performed by the stakeholder group. For instance, algorithmic approaches used by physicians facilitated timely diagnosis of CDI. Conflicting barriers or facilitators were related to opposing objectives; for example, clinicians needed rapid placement of a patient in a room while EVS staff needed time to disinfect the room.
Conclusions: A systems engineering approach can help to holistically identify factors that influence successful implementation of subprocesses of infection prevention bundles.
Conflict of interest statement
There is no conflict of interest to declare for any of the authors.
Figures
References
-
- Lucado J, Gould C, Elixhauser A. Clostridium Difficile Infections (CDI) in Hospital Stays, 2009: Statistical Brief #124 Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006. - PubMed
-
- Weiss K, Boisvert A, Chagnon M, et al. Multipronged intervention strategy to control an outbreak of Clostridium difficile infection (CDI) and its impact on the rates of CDI from 2002 to 2007. Infect Control Hosp Epidemiol 2009;30:156–162. - PubMed
-
- Evans ME, Kralovic SM, Simbartl LA, Jain R, Roselle GA. Effect of a Clostridium difficile Infection Prevention Initiative in Veterans Affairs Acute Care Facilities. Infect Control Hosp Epidemiol 2016;37:720–722. - PubMed
-
- McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 2018;66:e1–e48. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
