

Cardiovascular adverse events during treatment with darunavir-based regimens in an Italian observational study
- PMID: 31190745
- PMCID: PMC6526181
- DOI: 10.2147/DDDT.S180981
Cardiovascular adverse events during treatment with darunavir-based regimens in an Italian observational study
Abstract
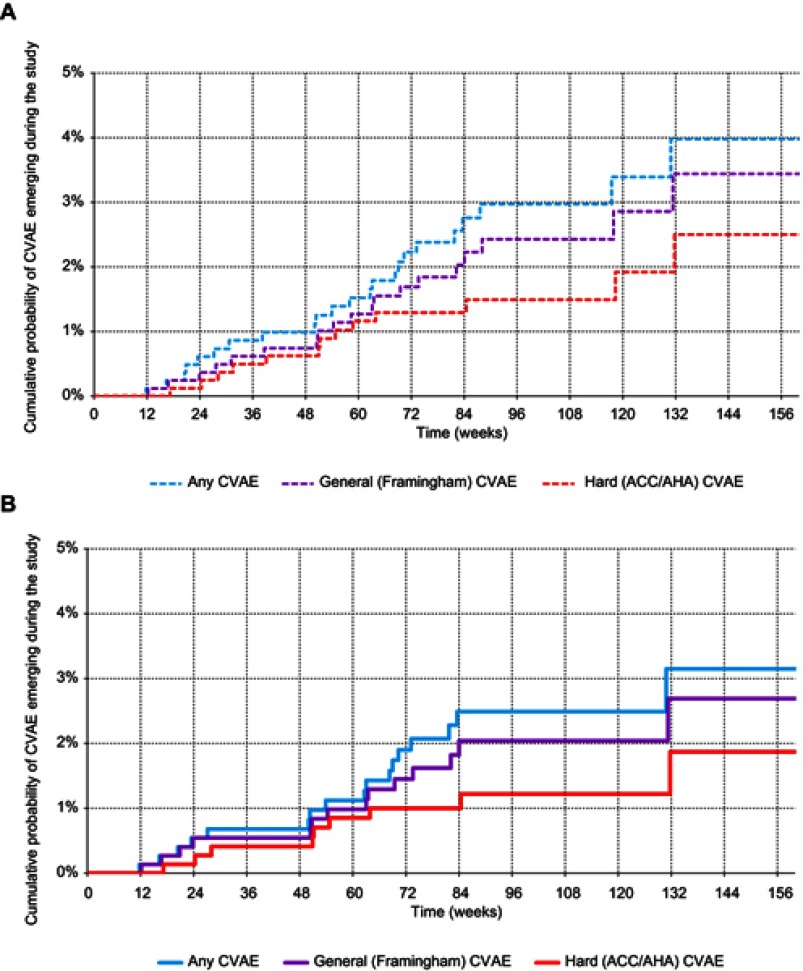
Background: The protease inhibitor (PI) darunavir (DRV) has proven to be highly effective and well tolerated for HIV treatment. The DAD (Data collection on Adverse Effects of Anti-HIV Drugs) cohort showed an increased 5-year cumulative cardiovascular (CV) risk in patients given various PIs, including DRV, whereas two other recent studies found no association between DRV and CV diseases. Methods: We performed a post-hoc analysis of CV adverse events (CVAEs) in an Italian cohort, the TMC114-HIV4042 observational study, where 875 patients treated with ritonavir-boosted DRV-based regimens were followed for a total of 1,566 patient-years. Results: We observed 23 CVAEs of any type, including 17 [12 (95%CI, 7-19) per 1,000 patient-years] primary; 14 [10 (95%CI, 5-17) per 1,000 patient-years] were primary Framingham-type general CVAEs, close to what expected according to the Framingham algorithm based on traditional risk factors. Age and systolic blood pressure (SBP) at the time of study enrolment were the only relevant (p<0.01) independent predictors of CVAEs in all models; patients with any CVAE were on average 10 years older and had an SBP 14 mmHg higher than patients without CVAEs. When controlling for age and SBP, the association with other traditional factors, including serum lipids, and with HIV-specific factors was not statistically significant (p>0.05). Models that also adjusted for previous ARV exposure showed no statistically significant association between any-type CVAEs and either DRV doses, 1,200 or 800 mg/daily (as also suggested by propensity score stratification), or previous DRV exposure duration. Conclusion : We found no evidence of a relationship between DRV use and increased CV risk.
Keywords: HIV infection; cardiovascular risk; darunavir; observational study.
Conflict of interest statement
A preliminary analysis of these data was accepted as oral presentation at 9th Italian Conference of AIDS and Antiviral Research (ICAR) 2017. The slides are available at the congress repository: http://www.icar2017.it/public/repository/slide/2_2_6_4_slide.pdf. A Antinori has received honoraria for consultancy with Gilead Sciences, ViiV Healthcare, Merck Sharp & Dohme, Janssen-Cilag, Abbvie, and Bristol-Myers Squibb and has also received research grants from Gilead Sciences, Bristol-Myers Squibb, Janssen-Cilag, and ViiV Healthcare. S Rusconi has received research funding from Pfizer and Janssen-Cilag and has been involved in advisory boards or educational courses supported by Abbvie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline, now ViiV Healthcare, Merck Sharp & Dohme, and Janssen-Cilag. N Gianotti has been advisor for Gilead Sciences, AbbVie, and Janssen-Cilag, received speakers’ honoraria from Gilead Sciences, ViiV Healthcare, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche, AbbVie, Boehringer Ingelheim, and Janssen-Cilag, and support for travel to meetings from Gilead Sciences, Bristol-Myers Squibb, AbbVie, Janssen-Cilag, Merck Sharp & Dohme, Roche, and ViiV Healthcare. T Bini has received research funding and/or honoraria from Merck Sharp & Dohme, Bristol-Myers Squibb, and Janssen-Cilag. D Mancusi and R Termini are employees of Janssen-Cilag SpA, Italy.
Figures
Similar articles
-
Effectiveness, durability, and safety of darunavir/ritonavir in HIV-1-infected patients in routine clinical practice in Italy: a postauthorization noninterventional study.Drug Des Devel Ther. 2016 May 6;10:1589-603. doi: 10.2147/DDDT.S104875. eCollection 2016. Drug Des Devel Ther. 2016. PMID: 27226708 Free PMC article.
-
Cardiovascular disease and use of contemporary protease inhibitors: the D:A:D international prospective multicohort study.Lancet HIV. 2018 Jun;5(6):e291-e300. doi: 10.1016/S2352-3018(18)30043-2. Epub 2018 May 3. Lancet HIV. 2018. PMID: 29731407
-
Virologic Effectiveness of Abacavir/Lamivudine with Darunavir/Ritonavir Versus Other Protease Inhibitors in Treatment-Experienced HIV-Infected Patients in Clinical Practice.Clin Drug Investig. 2017 Jan;37(1):51-60. doi: 10.1007/s40261-016-0456-1. Clin Drug Investig. 2017. PMID: 27587070 Free PMC article.
-
Darunavir: A Review in Pediatric HIV-1 Infection.Paediatr Drugs. 2015 Oct;17(5):411-21. doi: 10.1007/s40272-015-0146-0. Paediatr Drugs. 2015. PMID: 26323490 Review.
-
Contemporary protease inhibitors and cardiovascular risk.Curr Opin Infect Dis. 2018 Feb;31(1):8-13. doi: 10.1097/QCO.0000000000000425. Curr Opin Infect Dis. 2018. PMID: 29232276 Review.
Cited by
-
Darunavir and Cardiovascular Risk: Evaluating the Data to Inform Clinical Care.J Infect Dis. 2020 Feb 3;221(4):498-500. doi: 10.1093/infdis/jiz482. J Infect Dis. 2020. PMID: 31828327 Free PMC article. No abstract available.
References
-
- Eyawo O, Franco-Villalobos C, Hull MW, et al; Comparative Outcomes And Service Utilization Trends (COAST) study. Changes in mortality rates and causes of death in a population-based cohort of persons living with and without HIV from 1996 to 2012. BMC Infect Dis. 2017;17(1):174. doi:10.1186/s12879-017-2254-7 - DOI - PMC - PubMed
-
- Costagliola D, Potard V, Lang S, et al. Is the risk of myocardial infarction in PLHIV associated with atazanavir or darunavir exposure? AIDS 2018: 22nd International AIDS Conference, July 23–27; 2018; Amsterdam, Netherlands Abstract TUPEB087.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
