

Long-term cost and utility consequences of short-term clinically important deterioration in patients with chronic obstructive pulmonary disease: results from the TORCH study
- PMID: 31190781
- PMCID: PMC6524132
- DOI: 10.2147/COPD.S188898
Long-term cost and utility consequences of short-term clinically important deterioration in patients with chronic obstructive pulmonary disease: results from the TORCH study
Abstract
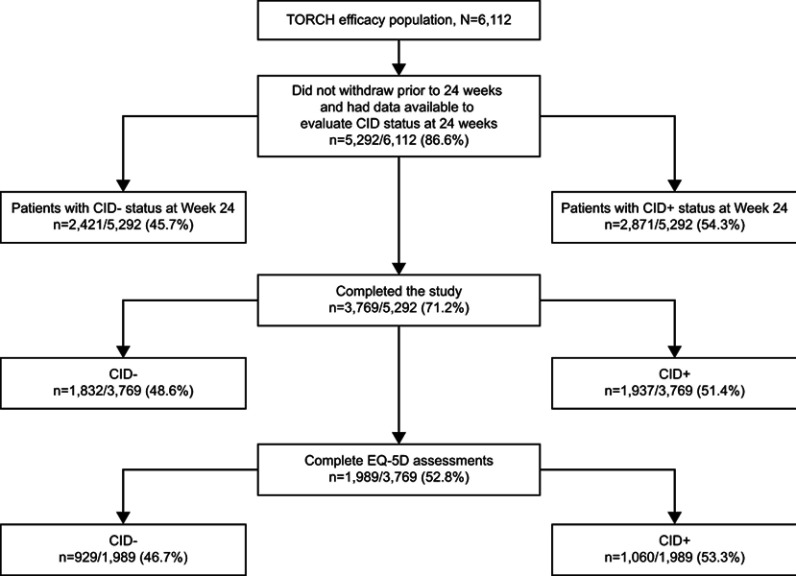
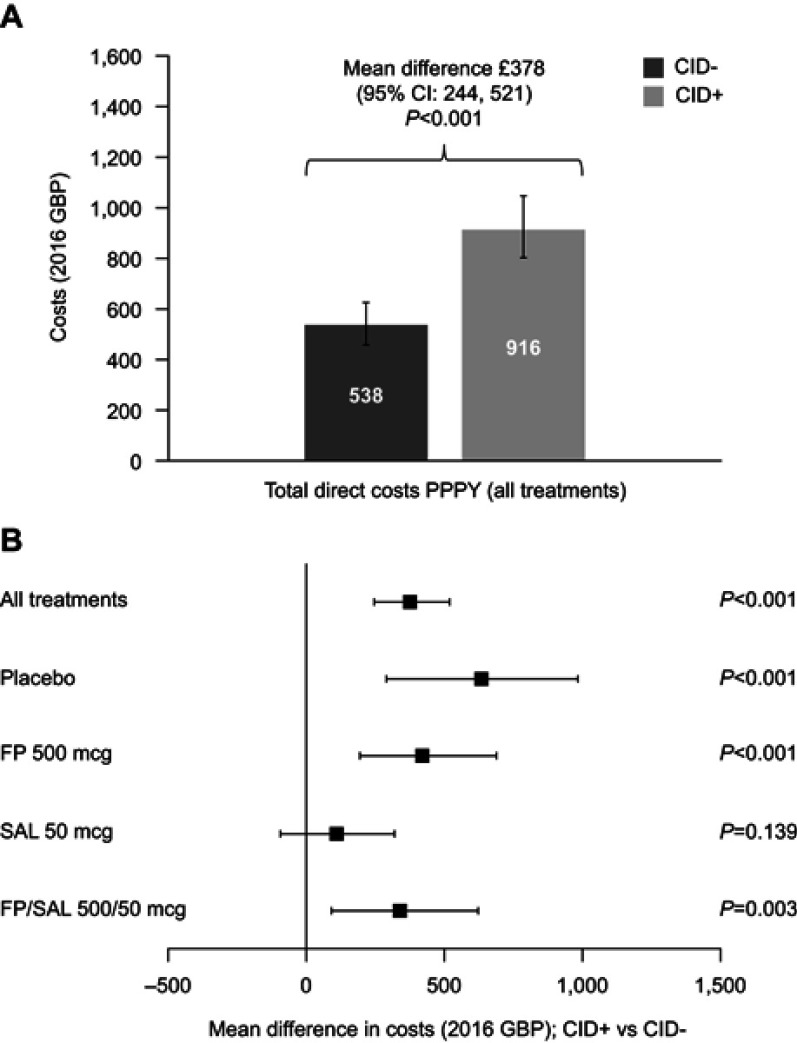
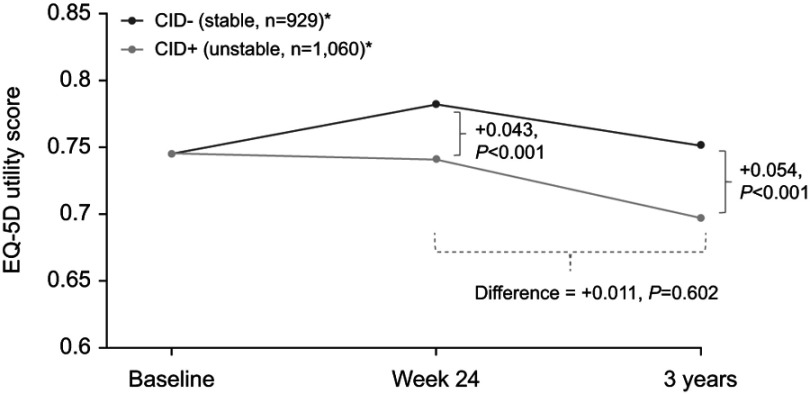
Purpose: Clinically important deterioration (CID) in chronic obstructive pulmonary disease (COPD) is a novel composite endpoint that assesses disease stability. The association between short-term CID and future economic and quality of life (QoL) outcomes has not been previously assessed. This analysis considers 3-year data from the TOwards a Revolution in COPD Health (TORCH) study, to examine this question. Patients and methods: This post hoc analysis of TORCH (NCT00268216) compared costs and utilities at 3 years among patients without CID (CID-) and with CID (CID+) at 24 weeks. A positive CID status was defined as either: a deterioration in forced expiratory volume in 1 second (FEV1) of ≥100 mL from baseline; or a ≥4-unit increase from baseline in St George's Respiratory Questionnaire (SGRQ) total score; or the incidence of a moderate/severe exacerbation. Patients from all treatment arms were included. Utility change was based on the EQ-5D utility index. Costs were based on healthcare resource utilization from 24 weeks to end of follow-up combined with unit costs for the UK (2016 GBP), and reported as per patient per year (PPPY). Adjusted estimates were generated controlling for baseline characteristics, treatment assignment, and number of CID criteria met. Results: Overall, 3,769 patients completed the study and were included in the analysis (stable CID- patients, n=1,832; unstable CID+ patients, n=1,937). At the end of follow-up, CID- patients had higher mean (95% confidence interval [CI]) utility scores than CID+ patients (0.752 [0.738, 0.765] vs 0.697 [0.685, 0.71]; difference +0.054; P<0.001), and lower costs PPPY (£538 vs £916; difference: £378 [95% CI: £244, £521]; P<0.001). The cost differential was primarily driven by the difference in general hospital ward days (P=0.003). Conclusion: This study demonstrated that achieving early stability in COPD by preventing short-term CID is associated with better preservation of future QoL alongside reduced healthcare service costs.
Keywords: EQ-5D; direct medical costs; resource utilization; utilities.
Conflict of interest statement
IN, NBG, and ASI are employees of GSK, and hold stock/shares in GSK. ASI is also an unpaid professor at McMaster University in Canada. MTD was employed by GSK at the time of this study. VFP and NR are employees of ICON Health Economics, who were contracted by GSK to conduct the study analysis. AB received consultancy fees from GSK and ICON Health Economics in relation to this study. AB and ICON employees were not paid for manuscript development. The authors report no other conflicts of interest in this work.
Figures

References
-
- Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2019. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14N.... Accessed December18, 2018.
-
- American Thoracic Society. The global burden of lung disease; 2014. Available from: http://foundation.thoracic.org/news/global-burden.php. Accessed August29, 2018.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
